
Dystonic tremor of the left upper limb revealing a neurocysticercosis of the right thalamus: a case report
Nomena Finiavana Rasaholiarison, Julien Razafimahefa, Lala Andriamasinavalona Rajaonarison, Alain Djacoba Tehindrazanarivelo
Corresponding author: Nomena Finiavana Rasaholiarison, Neurology Department, Andrainjato University Teaching Hospital, Fianarantsoa, Madagascar 
Received: 05 Feb 2024 - Accepted: 05 Mar 2024 - Published: 20 Mar 2024
Domain: Neurology (general)
Keywords: Case report, dystonic tremor, neurocysticercosis, thalamus
©Nomena Finiavana Rasaholiarison et al. PAMJ Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Nomena Finiavana Rasaholiarison et al. Dystonic tremor of the left upper limb revealing a neurocysticercosis of the right thalamus: a case report. PAMJ Clinical Medicine. 2024;14:28. [doi: 10.11604/pamj-cm.2024.14.28.42892]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com//content/article/14/28/full
Case report 

Dystonic tremor of the left upper limb revealing a neurocysticercosis of the right thalamus: a case report
Dystonic tremor of the left upper limb revealing a neurocysticercosis of the right thalamus: a case report
![]() Nomena Finiavana Rasaholiarison1,&,
Nomena Finiavana Rasaholiarison1,&, ![]() Julien Razafimahefa2, Lala Andriamasinavalona Rajaonarison3, Alain Djacoba Tehindrazanarivelo2
Julien Razafimahefa2, Lala Andriamasinavalona Rajaonarison3, Alain Djacoba Tehindrazanarivelo2
&Corresponding author
Dystonic tremor is often associated with a thalamic lesion, in rare cases this lesion can be a neurocysticercosis. Our objective was to report a case of dystonic tremor by neurocysticercosis in the right thalamus and to discuss the diagnosis and treatment. An 11-year-old Malagasy girl consulted for a progressive persistent movement disorder of the left upper and lower limbs. She was treated as an epileptic patient with no remission. On examination, she had a dystonic tremor of the left upper limb, kinesigenic dystonia of the left lower limb, hemiparesis, and amyotrophies of the left body side. Her cysticercosis serological test was positive. Her brain CT scan with injection showed a voluminous edematous annular image in the right posterior thalamus. The brain CT scan after treatment showed a calcification sequela of a thalamopedoncular neurocysticercosis. We should think about neurocysticercosis and perform a brain imaging in endemic areas when seeing movement disorders in children.

Dystonia is an abnormal movement characterized by sustained or intermittent muscle contractions causing often repetitive movements abnormal postures, or both. Dystonic tremor (DT), which is defined as a tremor in a part of the body affected by dystonia, gives spontaneous oscillatory, arhythmic, movements, although inconstant. Those movements are produced by contractions of dystonic muscles, often exacerbated by an attempt to maintain a primary (normal) posture [1-3]. This DT can be acquired (dystonia due to a known specific cause). It is frequently associated with a thalamic lesion and results from a dysfunction in the cerebello-thalamo-cortical pathway [1,4]. In rare cases, this lesion may be a neurocysticercosis, which is endemic to Madagascar. Abnormal movements secondary to neurocyticercosis are rare, although cysticercosis cysts localize in the basal ganglia in 25% of neurocysticercosis cases [3,5]. Neurocysticercosis and dystonic tremor have rarely been described in Madagascar, and can be difficult to manage. We report a case of dystonic tremor by neurocysticercosis in the right thalamus and discuss the diagnosis and treatment.

Patient information: it was an 11-year-old-girl from Madagascar with a past medical history of birth dystocia and chronic headaches of increasing intensity, but headaches remained steady after. She was followed in our unit for movement disorders of the left upper and lower limbs. Since the age of 7, she progressively developed irregular action tremors of the left upper limb. Then one year later the movement disorders worsened with action and postural dystonic tremors of the left upper limb and dystonia with torsion of the left lower limb (varis equina), leading to walking disorders. The left upper limb assumed a flexed attitude. She was treated as an epileptic with PHENOBARBITAL 2 mg/kg/day and SODIUM VALPROATE 25 mg/kg/day after a brain scan with microcrania and an EEG showing a partial epileptic seizure. Her mother stopped the treatment because the patient was sleepy, and no improvement was noticed. At the age of 9, a new brain CT scan with injection showed a voluminous edematous annular image in the right posterior thalamus. And the serological test for cysticercosis was positive. She was treated with ALBENDAZOLE at 8 mg/kg/day for 15 days, with corticosteroids at 1 mg/kg/day for 5 days. SODIUM VALPROATE was reintroducing at the same dose. She had no improvement. She was seen in consultation in our department 2 years later. She still presented abnormal movements on the left side with increased intensity, especially in cases of stress and emotion. She could not remain stable, had difficulties with school, and had enuresis. Her anti-epileptic drugs were taken off again.
Clinical findings: she had a flexion attitude of the left upper limb, with permanent postural/kinetic oscillation, sometimes resting, irregular with finger dystonia, not seen at complete rest. She spread her left index finger with her right hand to try to calm the dystonic tremors of the left upper limb (geste antagoniste) (Figure 1). She had left hemiparesis with amyotrophies. When she stood up and walked, she had a torsion of the left lower limb. She had no cerebellar syndrome, no cogwheel rigidity, and no rest tremor. No cysticercosis nodules in other parts of the body.
Timeline of current episode: since the age of 7 years old, the patient had dystonia treated as epilepsy but without improvement. At the age of 9 years old, she underwent a brain CT scan showing a neurocysticercosis on the right thalamus. So cysticidal was added to her treatment, but still, there was no improvement. Two years later she was seen in our neurology department and a dystonic tremor of the left upper limb and kinesigenic dystonia of the left lower limb was seen. The neurocysticercosis was localized on the right thalamus.
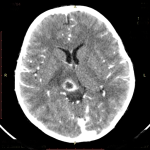
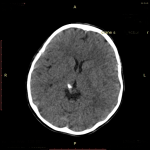
Diagnostic assessment and diagnosis: the dystonia of the patient was confirmed by a neurologist. The new brain CT scan with injection showing a voluminous edematous annular image in the right posterior thalamus (Figure 2) suggests neurocysticercosis lesion. Treatment with cysticidal and corticosteroids led to the improvement of the lesion. So, the last brain CT scan done two years after the treatment showed only a calcification as a sequela of thalamic neurocysticercosis (Figure 3).
Therapeutic interventions: the patient has received a cysticidal and corticosteroids to treat her neurocysticercosis. Anticholinergic, TROPATEPINE 20 mg/day was gradually introduced, with physiotherapy to treat her dystonia. Therapeutic education of the patient and family was done.
Follow-up and outcome of interventions: an improvement in the brain lesion was observed. The patient's abnormal movements didn´t disappear. The patient had no side effects of her anticholinergic drugs.
Patient perspective: the patient was satisfied to have the right diagnosis. She did not improve well with the anticholinergic treatment.
Informed consent: informed consent was obtained from the patient´s parents for us to use the case.
Movement disorders following neurocysticercosis are rare [5]. In our case, the patient presented a dystonic tremor (TD), and acquired dystonia of the left upper limb and the left lower limb with different intensity by a neurocysticercosis nodule in the right thalamic. The patient was seen late. Despite the treatment with corticosteroids, antiepileptic, anticholinergic drugs, and cysticidal, the patient's abnormal movements did not remit. As limitations in our case, a biopsy of the lesion, fundoscopy for cysticercosis nodule in the eyes, brain MRI for lesion accuracy and 6-month follow-up, CSF neurocysticercosis serology, stool larvae test, and chest X-ray were not performed. The patient could not afford them. Despite that, we treated the patient. We had an improvement in the brain scan. The patient's movement disorders did not go into complete remission. This situation is due to the residual calcification on the thalamus and other medications such as tetrabenazine and clonazepam have not yet been introduced. Botulinum toxin injection, surgical treatment, or deep brain stimulation are not yet available in Madagascar. The patient also experienced diagnostic wandering for a few years before being diagnosed.
Horisawa et al. presented a patient with dystonic tremors, which are postural and intentional tremors in his left hand. He also had stiffness in his left hand, which resulted in mild difficulty in opening his left hand [6]. Schneider et al. also described their patients' dystonic tremors as a thumb extension tremor or task- or position-specific tremor associated with head tremor, dystonic voice. The tremors are more asymmetric or unilateral, more specific to position and task, with more frequent involvement of the neck and dystonia in the affected limb [7]. In one case reported by Cáceres-Redondo et al. the patient presented a resting tremor and postural tremor in the arms with a slight dystonic posture of the right arm. The dystonic posture and tremor improved if she touched her right shoulder. During walking, bilateral arm swing was reduced, and she had dystonic posture in both legs [8]. In the case of Cho et al. they described a patient with dystonic tremor of the left upper limb due to ischemic injury to the anterior part of the right thalamus. In thalamic lesions, the tremors can be of attitude, action, and rest, associated with a contralateral hemiparesis to the thalamic lesion. They were predominant in the contralateral upper limb as well [9]. Alvarez et al. also presented a patient with focal dystonia of the right hand and a postural tremor of the affected limb. The tremor was resting and postural, which did not subside during action in the right upper limb, particularly involving the wrist, index finger, and proximal musculature when extending the arm against gravity. This tremor made it impossible to use the right upper limb for any activity. On imaging, the patient showed lesions in the posterolateral thalamus [10]. In a case series of 16 cases of dystonia described by Lee et al. all had unilateral lesions in the thalamus (the posterior posterolateral thalamus and three in the paramedian thalamus in most cases), 10 had contralateral hemidystonia, five had contralateral focal dystonia (all affecting the hand and/or arm), and one had segmental dystonia involving the contralateral face, arm, and hand. Eleven cases developed dystonia following stroke; eight were due to infarction and three to hemorrhage. Three cases were associated with head trauma and two cases with thalamotomy [4].
Dystonic tremor syndromes (DTS) include tremors and dystonia as the main neurological signs. Two types of tremor are generally distinguished in dystonia: dystonic tremor (DT), which is defined as a tremor of a body part affected by dystonia, and dystonia-associated tremor (DAT), defined as a tremor of a body part not affected by dystonia. The clinical features of dystonic tremor are coarse, jerky, irregular, directional, and asymmetric. The tremor began at or after the onset of dystonia in DT. Whereas the tremor began before the onset of dystonia in dystonia-associated tremor. DT showed less inhibition in the cerebello-thalamo-cortical pathway. A recent functional neuroimaging study showed that there was extensive cerebello-thalamo-cortical activity associated with tremors in DT. The latter may be difficult to distinguish from essential tremor [1-3]. All lesions of the thalamus do not result in abnormal movements, and the movement disorders are not necessarily dystonic tremors. This could be because brain imaging scans may underestimate the extent of pathological damage. Then, they do not detect the functional changes associated with anatomical damage. In addition, the clinical features and exact location of lesions are not described in detail in many reports. Finally, neurological impairment may not be directly due to the effects of the identified lesion or damaged structure but may represent the consequences of the release of other brain systems from the control of the lesioned area [4].
In the classification of dystonia, our case constitutes dystonia due to a known specific cause or acquired dystonia due to neurocysticercosis infestation [3]. Neurocysticercosis (NCC), is a parasitic disease caused by encysted larvae of Taenia solium. It is endemic to Madagascar. Although parasitic cysts localize in the basal ganglia in 25% of NCC cases, particularly in the putamen and caudate nuclei, abnormal movements secondary to NCC are rare. The mechanism responsible for the clinical manifestations of NCC was the inflammatory reaction surrounding the cyst. It is generally assumed that inflammation around a cysticercus marks the beginning of the cyst death process [5]. As in our patient. Horisawa et al. had a patient with dystonic tremor treated with trihexyphenidyl (6 mg), clonazepam (3 mg), propranolol (120 mg), primidone (750 mg), and L-dopa (300 mg) which proved ineffective. But deep brain stimulation at the level of the pallidothalamic tract almost completely improved the dystonia of the left hand and foot [6]. For Mario Alvarez et al. a thalamotomy at the level of the Intermediate Ventral Nucleus, was performed with intra-operative semi-micro recording to verify the target [10]. In our patient, dystonia was persistent because of the residual calcification on the thalamic region. And we can not perform surgery for this lesion. As for the cases above, our oral treatment was not so efficient.
Neurocysticercosis in the thalamus can lead to dystonia and dystonic tremor. It is a curable cause. These clinical manifestations and lesions are potentially reversible, if diagnosed and treated in time. Neurocycticercosis is among the infectious acquired causes of dystonia, especially in endemic countries as Madagascar. In fact, brain imaging with contrast is a key point of the diagnostic workup.
The authors declare no competing interests.
Patient management: Julien Razafimahefa. Data collection: Nomena Finiavana Rasaholiarison. Manuscript drafting: Nomena Finiavana Rasaholiarison. Manuscript revision: Lala Andriamasinavalona Rajaonarison and Alain Djacoba Tehindrazanarivelo. All authors approved the final version of the manuscript.
Figure 1: patient spreading her left index finger with her right hand to try to calm the dystonic tremors of the left upper limb (geste antagoniste)
Figure 2: a voluminous edematous annular image in the right posterior thalamus, in the axial section, on a brain CT scan with contrast injection
Figure 3: calcification as a sequela of thalamic neurocysticercosis in the axial section on CT scan without contrast injection
- Panyakaew P, Cho HJ, Lee SW, Wu T, Hallett M. The Pathophysiology of Dystonic Tremors and Comparison With Essential Tremor. Journal of Neurosci. 2020;40(48): 9317-9326. PubMed | Google Scholar
- Elble RJ. Defining Dystonic Tremor. Current Neuropharmacology. 2013 Jan;11(1):48-52. PubMed | Google Scholar
- Albanese A, Bhatia K, Bressman SB, DeLong MR, Fahn S, Fung VSC et al. Phenomenology and Classification of Dystonia: A Consensus Update. Mov Disord. 2013;28(7):863-87. PubMed | Google Scholar
- Lee MS, Marsden CD. Movement Disorders Following Lesions of the Thalamus or Subthalamic Region. Mov Disord. 1994;9(5):493-507. PubMed | Google Scholar
- Cosentino C, Ve'lez M, Torres L, Garcia HH. Neurocysticercosis-Induced Hemichorea. Mov Disord. 2006;21(2):286-7. PubMed | Google Scholar
- Horisawa S, Kohara K, Nonaka T, Mochizuki T, Kawamata T, Taira T. Case Report: Deep Cerebellar Stimulation for Tremor and Dystonia. Front. Neurol. 2021;12:642904. PubMed | Google Scholar
- Schneider SA, Edwards MJ, Mir P, Cordivari C, Hooker J, Dickson J et al. Patients With Adult-Onset Dystonic Tremor Resembling Parkinsonian Tremor Have Scans Without Evidence of Dopaminergic Deficit (SWEDDs). Mov Disord. 2007;22(15):2210-5. PubMed | Google Scholar
- Cáceres-Redondo MTC, Carrillo F, Palomar FJ, Mir P. DYT-1 Gene Dystonic Tremor Presenting as a ��Scan Without Evidence of Dopaminergic Deficit´´. Mov Disord. 2012;27(11):1469. PubMed | Google Scholar
- Cho C, Samkoff LM. A lesion of the anterior thalamus producing Dystonic Tremor of the hand. Arch Neurol. 2000 Sep;57(9):1353-5. PubMed | Google Scholar
- Àlvarez M, Quintanal N, Díaz A, Prince J, García I, Carballo M et al. Dystonia and Tremor Secondary to Thalamic Infarction Successfully Treated With Thalamotomy of the Ventralis Intermedius Nucleus. Mov Disord. 2014;29(9):1188-1190.. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures

Article metrics

