
Breast tuberculosis: a case report
Toumi Safae, Chenguiti Ansari Anas, Moutaa Ibtissam
Corresponding author: Toumi Safae, Department of Obstetrics and Gynecology, Souissi Maternity, Rabat, Morocco 
Received: 07 Feb 2022 - Accepted: 11 Mar 2022 - Published: 08 Apr 2022
Domain: Gynecology
Keywords: Breast, tuberculosis, antibacillary, mastodynia, case report
©Toumi Safae et al. PAMJ Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Toumi Safae et al. Breast tuberculosis: a case report. PAMJ Clinical Medicine. 2022;8:53. [doi: 10.11604/pamj-cm.2022.8.53.33643]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com//content/article/8/53/full
Case report 

Breast tuberculosis: a case report
Breast tuberculosis: a case report
![]() Toumi Safae1,&, Chenguiti Ansari Anas1, Moutaa Ibtissam1
Toumi Safae1,&, Chenguiti Ansari Anas1, Moutaa Ibtissam1
&Corresponding author
Breast is one of the least common location for tuberculosis (TB) infection, without any evident guidelines for both clinical and paraclinical diagnosis. In this paper, we illustrate a case report of a patient who presented with primary mammary tuberculosis and, through the data in the literature, we focus on the different aspects of this pathology. Mammary tuberculosis is a heavy pathology mainly by the duration of the treatment and its sequelae, hence the interest of prevention, early diagnosis and treatment.

Breast tuberculosis is a rare but prevalent form (especially in endemic countries) of extra-pulmonary tuberculosis. This localization in the breast can be primary or secondary, and it often causes diagnosis issues both clinical and paraclinical.

Patient information: our patient is 27 years old women, married and mother of two, born and raised in an urban zone (Rabat), with no particular medical history who presented to our consultation with an increase of the volume of the right breast after weaning from breastfeeding, with mastodynia and without associated nipple discharge.
Clinical findings: the initial physical examination finds a poorly limited painful mass of the right breast without other associated signs.
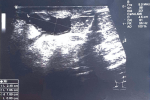
Diagnostic assessment: on ultrasonography, a roughly oval formation of the LIQ of the right breast was highlighted in favor of an impure cyst measuring 12.5 mm x 22.5 mm. In the absence of clinical improvement, the patient underwent ta second ultrasonography showing (Figure 1, Figure 2). Presence in retro-areolar of two poorly limited fluid collections, with an infiltration of the adjacent fatty tissue, seeming to communicate with each other by a fistulous path. These collections measure: 25 x 10 mm and 17 x 11 mm. Discrete right galactophoric dilation with echogenic content.
Diagnosis: a biopsy of the right breast was carried out; showing Specific inflammatory granulomatous changes primarily suggesting a tuberculous origin.
Therapeutic interventions: the patient was referred to the tuberculosis diagnosis and treatment center for anti-tuberculosis treatment: ERIP K4 (RHZE): for 2 months then RH 300 for 4 months with good clinical progress and the breast control ultrasound was without particularities.
Follow-up and outcome of interventions: three years later, the patient consults for bilateral mastodynia and unilateral bloody breast discharge relapse on the same breast. The patient resumes the same anti-tuberculosis protocol for 6 months and the control ultrasound showed a slight regression in size of most of the hypoechoic right breast formations (Figure 3), one of which has a slight increase in size (UIQ). The patient reports good overall evolution with persistence of sequelae mastalgia leading her to consult every 6 months for 2 years.
Informed consent: the patient provided her full consent after oral explanation of our intention of publishing her case.
This tuberculous localization is presented either as an isolated attack or associated with other bacillary, ganglionic, osteo-articular or genitourinary attacks. This makes it possible to distinguish two types of breast tuberculosis:
Primary mammary tuberculosis: it is a form where tuberculosis is initially localized in the breast. It is clearly the most frequent and represents 60% of cases. To some authors it is most likely associated with other tuberculous foci, mainly pulmonary scarring and intercostal lymph nodes, that were not detected before [1,2].
Secondary breast tuberculosis: less frequent form than the primitive, it follows the prior involvement of an organ other than the breast. Bacillary extension can be done in four ways: 1) the lymphatic route: the most common mode of extension, by which the dissemination of KB takes place from mediastinal, cervical, supraclavicular or axillary lymphadenopathy [3]; 2) the hematogenous route: rarely described, mostly dependent on the structure of the mammary gland where tuberculosis presents a lobular and ductal distribution as in the lung [4]; 3) penetration from the nipple through the milk ducts is a possible route of contamination by the dilation of the milk ducts in women during pregnancy and lactation [5]; direct extension from adjoining organs occurs by contiguity from cutaneous, pleural or osseous localizations [4].
Concerning the clinical aspects, breast tuberculosis is mastitis, the onset of which is insidious and nonspecific. The lesions are often unilateral and mainly occur in the upper external quadrant. According to Wilson and MacGregor, bilaterality is observed in only 3% of cases [6]. In young women, mammary tuberculosis mimics a pyogenic abscess and, in older women, mammary carcinoma [7].
Three clinical forms are usually described: 1) nodular form: this is the most frequent one, representing 76.8% of cases. It manifests clinically by a circumscribed swelling of variable size, associated or not with lymphadenopathy [8]; 2) diffuse form: it usually succeeds a nodular form if it has not been treated, and represents 11.2% of mammary tuberculosis [9]. Clinically, it is a painful, poorly limited swelling that can extend over the entire gland and adhere to the skin with, sometimes, a bloody or purulent discharge, anappearance clinically reminiscent of carcinomatous mastitis; 3) sclerotic form: it accounts for 1.4% of breast tuberculosis and mainly affects elderly women. It is characterized by an appearance of tuberculous squirrhe, which makes it possible to differentiate it from a squirrhous cancer. This squirrhe retracts the breast against the costal grill, thus giving the appearance of a reduced breast size, suppuration is very rarely noted [8].
The pathological examination performed on biopsies or lumpectomy pieces remains the decisive argument for mammary tuberculosis, showing epitheloid follicles and giant Langhans-type cells with caseous necrosis. The presence of a tuberculoid lesion with an incomplete or rough follicle could correspond to other granulomatous disorders, such as leprosy or sarcoidosis of the breast [10]. The observation of necrotizing granulomatous inflammation, composed of epithelioid histiocytes follicles, is not always pathognomonic of tuberculosis. Indeed, some granulomatous mastitis with non-tuberculous caseous necrosis, in particular cryptococcosis,plasmacytosis, tularemia, blastomycosis, histoplasmosis, and the giant cell reactionon foreign bodies have the same histological appearance, in these cases, the bacteriological study is necessary.
Bacteriological proof is made either by the demonstration of KB, by direct examination or by culture, and is based on the discovery of Mycobacterium tuberculosis in the fine needle aspiration fluid or in a sample of pus. Ziehl's stain can almost immediately confirm the tuberculous nature of the breast infection, but it is often by culturing the sample that the bacteriological diagnosis is made. Nucleic acid amplification (NAAT) assays such as polymerase chain reaction (PCR) are rapid and specific, but suffer from low sensitivity, especially in smear negative cases. Sensitivity as low as 50% has been reported in some series. This low sensitivity is due to the presence of polymerase inhibitors in approximately 20% of extrapulmonary samples. Thus, a negative NAAT result does not exclude TB disease with certainty.
The differential diagnosis of mammary tuberculosis arises with the clinical and radiological aspects of breast cancer and that of benign mastopathies, in particular fibroadenoma and phyllodes tumor [8].
The differential diagnosis occurs mainly with: 1) Breast cancer: this diagnosis is the first to rule out, especially in elderly women, due to the fact that clinical and radiological similarity are quite important [11,12]. Mammary Paget's disease: classically presents in the form of an eczema-like itchy plaque in the nipple region, most often unilateral. Only a histological study would allow to retain the diagnosis of mammary tuberculosis [10]. Benign breast mastopathies: represent the main problem of differential diagnosis in young women, it is of varying difficulty depending on whether the mastitis progresses acutely or chronically [8].
Histologically
It is possible to discover, during certain mammary inflammatory syndromes, typically granulomatous histological formations confusing with mammary tuberculosis. These syndromes are dominated by: sarcoidosis, ductal ectasia, cytosteatonecrosis and idiopathic granulomatous mastitis and chronic plasma cell mastitis [13]. In the literature, cases associating cancer and mammary tuberculosis have been described, hence the need for a histological study of the mammary tissue in order to eliminate an associated carcinoma.
The treatment of mammary tuberculosis is identical to that of other extrapulmonary tuberculosis sites. It consists of a combination of antibacillary chemotherapy for six months. Surgery can be associated with this medical treatment, during which drainage of suppurative collections and excision of necrotic tissue will be performed. This treatment is only initiated after bacteriological or histological proof. The anti-tuberculosis drugs are isoniazid, rifampicin, pyrazinamide, ethambutol and streptomycin. The principles of treatment against breast tuberculosis are based on the combination of two active drugs, treatment must always be prolonged (six to 18 months depending on the clinical context and the scheme followed), at an effective and adequate dose. medication is taken only in the morning, on an empty stomach and on a daily basis (six days a week). The antibacillary regimen followed in all our patients was based on triple therapy for two months (rifampicin + isoniazid + pyrazynamide), followed by dual therapy for a period of four months (rifampicin + isoniazid).
Since the advent of antibiotics, the place of surgery remains limited. the surgical act allows biopsies, excisions and lumpectomies to be performed in order to have histological proof of breast tuberculosis. In addition, surgery turns out to be necessary in addition to medical treatment in certain cases, in particular to drainabscesses, resection (as much as possible) of necrotic and infected tissue, resection of a nodule when it exists, a mastectomy when the lesions are extensive and the breast is completely destroyed and riddled with fistulas or to remove residual lesions after medical treatment.
When it comes to the prognosis, locally; untreated breast tuberculosis has a poor prognosis, as it will eventually invade the entire breast; the disease can spread to the posterior wall of the gland, thus collapsing the chest wall and pleural space. The evolution is most frequently towards suppuration. It is done either slowly or accelerated by pregnancy or breastfeeding. Mastitis softens to become fluctuating. Its puncture brings back a pus rich in BK which makes it possible to start the anti-bacillary treatment early, avoiding the appearance of fistulization. If the lump is left on its own, a cold intra-mammary abscess that eventually adheres to the skin causing the nipple to retract, leaving after partial evacuation, a characteristic chronic tuberculous fistula with a single orifice or more frequently multiple ones.
Finally, the breast becomes irregular, bumpy, fistulized at several points. These fistulas will become purplish, leaving the caseum to weld and have little or no tendency to heal. In elderly women, especially we see the disease at the stage of sclerosis, the mammary lesion is the seat of a fibrous process which remains localized or on the contrary extends to the entire gland. This gradually takes on the appearance of a squirrhe [14]. When treatment is early and well conducted, breast tuberculosis has a good prognosis in most cases. The recurrence can be local, at the level of the axillary hollow or on the opposite side, following inadequate antibacillary treatment or non-compliance with the treatment by the patient. The vital prognosis depends on the other tuberculous sites. These extramammary locations can be progressive or quiescent.
Breast tuberculosis is a rare extra-pulmonary localization of tuberculosis, the diagnosis of which can create some difficulties, both clinical and paraclinical. It will only be confirmed by the histological study of the biopsies which will show the specific lesions the essential differential diagnosis being breast cancer, must not be overlooked. Despite its rarity, this diagnosis should frequently be mentioned in countries with a tuberculosis endemic profile.
The authors declare no competing interests.
All the authors have read and agreed to the final manuscript.
Figure 1: ultrasonography of a retro-areolar fluid collection
Figure 2: ultrasonography of a poorly limited fluid collection with an infiltration of the adjacent fatty tissue
Figure 3: ultrasonography of a slight regression in size of most of the hypoechoic right breast formations
- Khaled A, Sâadi A, Jaziri M, Ben Romdhane K, Boussen H, Khattech R et al. La tuberculose mammaire: aspects radio-cliniques: à propos de 70 cas. Rev Im Med. 1992;4:755-8.
- Banerjee SN, Ananthakrishnan N, Mehta RB, Parkash S. Tuberculous mastitis: a continuing problem. World J Surg. 1987;11(1):105-109. PubMed | Google Scholar
- Zandrino F, Monetti F, Gandolfo N. Primary tuberculosis of the breast. A case report. Acta Radiol. 2000;41(1):61-63. PubMed | Google Scholar
- Thimmappa D, Mallikarjuna MN, Vijayakumar A. Breast Tuberculosis. Indian J Surg. 2015;77(Suppl 3):1378-1384. PubMed
- Hawilo A, Abdelmalek R, Mebazaa A, Addouni O, Kanoun F, El Euch D et al. La tuberculose mammaire: un diagnostic rare, souventméconnu. Med Sante Trop. 2012;22(3):292-296. PubMed | Google Scholar
- Sarah T, Slaouoi A, Benzina I. Primary breast tuberculosis. Surg Case Rep. 2020;4(1):3-5.
- Tazzioli G, Macolino A, Combi F et al. Breast tuberculosis: a case report of primary type mammary tuberculosis. Clin Case Rep. 2019 Oct 23;7(12):2346-2348. PubMed | Google Scholar
- Ben Hassouna J, Gamoudi A, Bouzaiene H, Palma E, Papi S, Codeluppi M et al. Tuberculose mammaire: étude rétrospective de 65 cas. Gynecol Obstet Fertil. 2005;33(11):870-876. PubMed | Google Scholar
- Daali M, Hssaida R, Hda A. La tuberculose primitive du sein. Presse Med. 2001;30(9):431-433. PubMed
- Salem A, Mnif N, Karray M, Kribi L, Ellouze T, Hamza R. Double localisationtuberculeusemammaire et rachidienne: à propos d'un cas. J GynecolObstet Biol Reprod (Paris). 2004;33(2):148-150. Google Scholar
- Soto C, Vizcaíno I, Isarria S, Pastor MR. Tuberculosis of the breast: imaging findings in two patients. Radiologia. 2008;50(6):518-521. PubMed | Google Scholar
- D'Souza MM, Tripathi M, Shrivastav M, Sharma R, Mondal A. Tuberculosis mimicking malignancy. Hell J Nucl Med. 2009;12(1):69-70. PubMed
- Salem A, Bennaceur R, Driss M, Mehiri S, Mrad K, Rajhi H et al. Imaging of granulomatous mastitis. Image Female. 2008;18:46-54.
- Hawilo A, Abdelmalek R, Mebazaa A, Addouni O, Kanoun F, El Euch D et al. Tuberculosis of the breast: a rare often unrecognized diagnosis. Médecine et Santé Tropicales. 2012;22(3):292-296. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures


Article metrics
PlumX Metrics
Breast tuberculosis: a case report
