
Mediastinal bronchogenic cyst revealed by acute epigastralgia: a case report
Fatima Belabbes, Oussama Afandi, Najwa Benslima, Jihane Habi, Sara Mounsif, Nada Faquir, Mohammed Reda El Ochi, Mouhammed Allaoui, Abderrahmane Al Bouzidi, Fedoua Rouibaa
Corresponding author: Fatima Belabbes, Department of Gastroenterology and Proctology, Cheikh Khalifa International University Hospital, Casablanca, Morocco 
Received: 30 Mar 2021 - Accepted: 03 Aug 2022 - Published: 08 Aug 2022
Domain: Gastroenterology, Thoracic surgery
Keywords: Bronchogenic, mediastinal tumor, cyst, thoracoscopy, case report
©Fatima Belabbes et al. PAMJ Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Fatima Belabbes et al. Mediastinal bronchogenic cyst revealed by acute epigastralgia: a case report. PAMJ Clinical Medicine. 2022;9:31. [doi: 10.11604/pamj-cm.2022.9.31.29102]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com//content/article/9/31/full
Case report 
Mediastinal bronchogenic cyst revealed by acute epigastralgia: a case report
Mediastinal bronchogenic cyst revealed by acute epigastralgia: a case report
Fatima Belabbes1,2 &, Oussama Afandi2,3, Najwa Benslima2,4, Jihane Habi2,4, Sara Mounsif1,2, Nada Faquir1,2, Mohammed Reda El Ochi2,5, Mouhammed Allaoui2,5, Abderrahmane Al Bouzidi2,5, Fedoua Rouibaa1,2
&Corresponding author
Bronchogenic cyst (BC) occurs as an abnormality in the development of the primary foregut and may be mediastinal or pulmonary in the location. Most patients remain asymptomatic for several years. We report the observation of a young patient, who presented a symptomatic bronchogenic cyst revealed by acute epigastralgia, without other associated signs. He underwent a chest computed tomography (CT) scan which showed a posterior mediastinal cystic formation and an oesogastric digestive uppergastro-intestinalendoscopy which showed an aspect of extrinsic compression with normal-appearing mucosa. The patient was operated on urgently. The operative procedure consisted of partial resection. The anatomopathological study of the surgical specimen confirmed the diagnosis. Through the presentation of this case, we wish to underline the rarity of this symptomatology and its sudden installation. This is a case to sensitize gastroenterologists to think of a bronchogenic cyst in acute abdominal pain and not to hesitate to ask for imaging.

Bronchogenic cysts are benign cystic tumors of embryonic origin [1]. They result from an abnormality in the development of an aberrant bud from the primary anterior intestine, or from the tracheobronchial outline and not having resulted in alveolar differentiation [1]. Their topography is mainly mediastinal in 36 to 90% of cases. However, they can stay at the level of the pulmonary parenchyma. Other rarer ectopic locations have been reported [2]. We report the case of a young patient, presenting a symptomatic bronchogenic cyst revealed by acute epigastralgia through which we try to underline the rarity of this symptomatology and its sudden onset, to emphasize the pathogenic theories concerning its embryological origin, its diagnosis and management.

Patient information: a 27-year-old man with no specific medical or surgical, presented an intense continuous acute epigastralgia of sudden installation, associated with clear vomiting. The patient reported no melena, dysphagia or transit disorders. He did not have anorexia, weight loss, fever, or asthenia. The patient has never previously presented the same symptomatology.
Clinical findings: general examination found a conscious apyretic patient that was hemodynamically and respiratory stable, normo-colored conjunctiva, without signs of extracellular or intracellular dehydration. Abdominal examination found a soft abdomen, without a palpable mass, and without dullness. The digital rectal examination was normal. The rest of the clinical examination, particularly respiratory and cardiovascular, were normal.
Diagnostic assessment: the results of the laboratory investigations were normal: no hydro-electrolyte disturbance, normal lipasemia, liver function tests were normal.
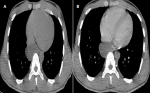
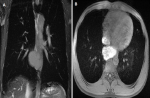
Imaging and endoscopic investigations: a chest radiograph was practiced first and was non-pathologic (Figure 1). Computed tomography examination was performed and showed a right middle mediastinal cyst, rounded, well limited, hypodense, without enhance after contrasts´ injection. It compresses the esophagus and the auricular cavity (Figure 2). A characterization magnetic resonance imaging (MRI) was performed to characterize the lesion and revealed the protein content of the cyst in hyper signal T1 and hyper signal T2 (Figure 3), which confirmed the diagnosis of bronchogenic cyst.
Esogastroduodenal endoscopy revealed an extrinsic esophageal compression with a rounded soft swelling of about 3 cm in diameter, located in the mucous membrane, bulging into the esophageal lumen and pushing back the mucous membrane which had a normal appearance. There was also an erythematous antrofundic gastritis and ulcerated bulbitis. An esophageal biopsy of this incidentally discovered lesion was taken but was not contributory. Gastric biopsy revealed an Helicobacter pylori gastritis.
Diagnosis: computed tomography examination and digestive endoscopy revealed esophageal compression by a large bronchogenic cyst.
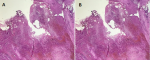
Therapeutic intervention: the patient was operated on urgently by a short right posterolateral thoracotomy passing through the 6 intercostal spaces, after a selective intubation with a gastric tube. Several important adhesions were found, making the dissection difficult. The cyst was opened and the contents were aspirated, then a sample was sent for bacteriological study. Partial resection of the cyst with coagulation of the mucous membrane at the bottom of the cyst were performed. A methylene blue test was carried out and was negative. A chest tube was placed and kept for 3 days. The early post-operative follow-up was normal. The anatomopathological study of the resected specimen confirmed the diagnosis (Figure 4).
Follow-up and outcomes: the surveillance scan after one week revealed a significant decrease in cystic volume (Figure 5).
Patient perspective: during hospital stay and at discharge, the patient's mother was very satisfied with the care.
Informed consent: informed consent was obtained from the patient for us to use the case.
Bronchogenic cysts are homoplastic dysembryomas whose wall is bronchial type, lined on its inner side with epithelium respiratory ciliate secreting mucus causing thick fluid contents [3]. Mediastinal bronchogenic cysts represent 8-10% of all surgical tumors of the mediastinum [3]. About 7 to 20% of mediastinal bronchogenic cysts depending on the series are closely related to the esophagus [3], with a large predominance of extramural cysts over intramural cysts. They affect both sexes and all ages. However, two recent studies (the KO et al. series and the turkilmaz series) have shown that it is predominant in young women with an average age of 29.9 [4].
Whether they are intra or extra-mural, bronchogenic cysts of the esophagus are asymptomatic and discovered by chance in half of the cases [5]. In our observation, the bronchogenic cyst was symptomatic. Numerous studies have shown that asymptomatic bronchogenic cysts become symptomatic over time and the symptoms can sometimes be very serious making surgery urgent. Intramural bronchogenic cysts of the esophagus can present with complications. Indeed, the natural history of bronchogenic cysts is to evolve into complications, especially infectious ones [6]. The diagnosis is mainly based on computed tomography (CT) and magnetic resonance imaging (MRI). The computed tomography (CT) scan guides the diagnosis by analyzing the topography, size and density of the cyst. The bronchogenic cyst is often located in the posterior mediastinum in 70% of cases, of rounded shape and of fluid or protein density [3]. Thanks to its different sequences, magnetic resonance imaging (MRI) is the gold standard in imaging. It improves the characterization of the cyst (its wall, and its content) as well as its environment. The wall of the cyst is thin. The contents are often aqueous (hypo signal T1, hyper signal T2). Sometimes, the content is rich in protein as in the case we are presenting (hyper signal T1 and T2) [7]. Endoscopic ultrasound is used in the assessment of paraesophageal locations [8]. It has been proposed as a common modality for diagnosis of cystic lesions of the esophagus. In chest X-rays, the bronchogenic cyst is classically manifested by mediastinal opacity or it can be normal if the lesion is small [9].
Surgical excision is generally recommended [10]. Complete surgical excision of the cyst is the only curative treatment [4]. The short posterolateral thoracotomy on the side where the cyct is predominantly located is the classic way to do it [9]. Maintaining the integrity of the cyst facilitates wall dissection and complete resection [5]. In the event of significant adhesions to "noble" organs (tracheal membrane, pulmonary veins, left atrium...) [11], it is classic to abandon an "egg cup" of the cyst. Video-assisted thoracoscopic surgery should be the first choice of treatment in adults with asymptomatic mediastinal bronchogenic cysts [6]. These lead to incomplete resections with the risk of subsequent recurrence, in other cases they are responsible for heavy surgery with removal of an entire lobe [12]. The difficulties encountered by the surgeon when the cyst is infected or inflammatory are often significant, the per and postoperative complications are very frequent [13]. The evolution in general is favorable and the postoperative effects are simple, but monitoring is essential.
Bronchogenic cysts are cystic dysembryomas that fit into the spectrum of bronchopulmonary malformations. In the majority of cases they are asymptomatic and the discovery is made during a systematic radiological assessment. However, bronchogenic cysts are mainly manifested by their complications which can be mechanical, infectious or hemorrhagic. The diagnosis of certainty remains anatomo-pathological. Surgical excision is also indicated for asymptomatic forms. The particularity of our case is the unusual symptoms of bronchogenic cyst, without previous episodes of crisis. It is necessary to think of an extra digestive cause in case of acute abdominal pain, in particular a bronchogenic cyst, to facilitate early diagnosis, and to improve patient’s management.
The authors declare no competing interest.
Patient management: FB performed the gastroscopy; JH and NB analyzed and interpreted the data from the MRI; OA operated on the patient; AA, MA and MO studied the anatomopathology of the kyst; data collection: FB, SM and NF; manuscript drafting: FB, OA and NB; manuscript revision: FB, FR, OA and NB. All the authors have read and agreed to the final manuscript.
Figure 1: normal chest X-ray of a 27-year-old patient who suffered from sudden epigastralgia with vomiting
Figure 2: the axial section of chest CT scan images: A) with and; B) without contrats´ injection, showing an enhanced right mediastinal cyst compressing the oesophagus and auricular cavity (white arrow)
Figure 3: mediastinal MRI of the bronchogenic cyst showing: A) thin-walled formation abutting to the oesophagus, its content is a hyper signal in a coronal section in weighted sequence T2; B) and a hyper signal in an axial section in weighted sequence T1 with fat saturation (white arrow)
Figure 4: A) the cyst is lined with a largely abraded coating and replaced by a polymorphic inflammatory infiltrate rich in histiocytes and polymorphs (HE, Gx200); B) cystic cavity with inflammatory and hemorrhagic wall (HE, Gx 50)
Figure 5: CT scan after surgical intervention (white arrow): significant decrease in the volume of the bronchogenic cyst
- Baccialone J, Le Bivic T, Jancovici R, Jeanbourquin D, Kremer S, Girodeau A et al. Les kystes bronchogéniques de l´adulte: histoire naturelle, revue générale, imagerie et actualités thérapeutiques. EM-Consulte. 2002;42(1):3-18. Google Scholar
- Maier HC. Bronchiogenic cysts of the mediastinum. Ann Surg. 1948;127(3):476-502. PubMed | Google Scholar
- Le Pimpec-Barthes F, Cazes A, Bagan P, Badia A, Vlas C, Hernigou A et al. Mediastinal cysts: clinical approach and treatment. Rev Pneumol Clin. 2010;66(1):52-62. PubMed | Google Scholar
- Binta BF, Othmane A, Mukenge T, Benmassaoud Z, Abdelhalim M, Khalid K et al. Les malformations pulmonaires congénitales: une expérience de 11 ans du service de chirurgie pédiatrique du CHU Hassan II de Fès. Pan African Medical Journal - Clinical Medicine. 2022;9:3.
- Turkyilmaz A, Eroglu A, Subasi M, Findik G. Intramural esophageal bronchogenic cysts: a review of the literature. Dis Esophagus. 2007;20(6):461-5. PubMed | Google Scholar
- Lakranbi M, Fenane H, Maidi Y, Msougar M, Ouadnouni Y, Bouchikh M et al. Kyste para-œsophagien révélé par des broncho-pneumopathies récidivantes. Rev Mal Respir. 2009 Nov;26(9):994-7. PubMed | Google Scholar
- Syed IS, Feng D, Harris SR, Martinez MW, Misselt AJ, Breen JF et al. MR imaging of cardiac masses. Magn Reson Imaging Clin N Am. 2008 May;16(2):137-64. PubMed | Google Scholar
- Jenssen C, Alvarez-Sánchez MV, Napoléon B, Faiss S. Diagnostic endoscopic ultrasonography: assessment of safety and prevention of complications. World J Gastroenterol. 2012 Sep 14;18(34):4659-76. PubMed | Google Scholar
- Hassaine A, Elbousaadni Y, Amrani R, Messaoudi S, Benhaddou H, Kamaoui I et al. Le kyste bronchogénique médiastinal: à propos d´un cas. 2018;4(10):194-196. Google Scholar
- Wang X, Chen K, Li Y, Yang F, Zhao H, Wang J. The video-assisted thoracic surgery for mediastinal bronchogenic cysts: a single-center experience. World J Surg. 2018;42(11):3638-45. PubMed | Google Scholar
- De Giacomo T, Diso D, Anile M, Venuta F, Rolla M, Ricella C et al. Thoracoscopic resection of mediastinal bronchogenic cysts in adults. Eur J Cardiothorac Surg. 2009 Aug;36(2):357-9. PubMed | Google Scholar
- Weber T, Roth TC, Beshay M, Herrmann P, Stein R, Schmid RA. Video-assisted thoracoscopic surgery of mediastinal bronchogenic cysts in adults: a single-center experience. Ann Thorac Surg. 2004;78(3):987-91. PubMed | Google Scholar
- Patel SR, Meeker DP, Biscotti CV, Kirby TJ, Rice TW. Presentation and management of bronchogenic cysts in the adult. Chest. 1994;106(1):79-85. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures


Article metrics

