
Cardiac tamponade and right pleural effusion secondary to amoebic liver abscess treated with repeated ultrasound guided-percutaneous needle aspiration: a case report
Sheikh Omar Bittaye, Saydiba Tamba, Musa Cham, Mariam Jaw, Ramou Njie
Corresponding author: Sheikh Omar Bittaye, Department of Internal Medicine, Edward Francis Small Teaching Hospital, Banjul, the Gambia 
Received: 25 Nov 2022 - Accepted: 03 Jan 2023 - Published: 06 Jan 2023
Domain: Cardiology,Gastroenterology,Infectious disease
Keywords: Amoebic liver abscess, cardiac tamponade, pleural effusion, case report
©Sheikh Omar Bittaye et al. PAMJ Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Sheikh Omar Bittaye et al. Cardiac tamponade and right pleural effusion secondary to amoebic liver abscess treated with repeated ultrasound guided-percutaneous needle aspiration: a case report. PAMJ Clinical Medicine. 2023;11:11. [doi: 10.11604/pamj-cm.2023.11.11.38352]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com//content/article/11/11/full
Case report 

Cardiac tamponade and right pleural effusion secondary to amoebic liver abscess treated with repeated ultrasound guided-percutaneous needle aspiration: a case report
Cardiac tamponade and right pleural effusion secondary to amoebic liver abscess treated with repeated ultrasound guided-percutaneous needle aspiration: a case report
![]() Sheikh Omar Bittaye1,2,&, Saydiba Tamba1, Musa Cham1,
Sheikh Omar Bittaye1,2,&, Saydiba Tamba1, Musa Cham1, ![]() Mariam Jaw1,2, Ramou Njie1,2
Mariam Jaw1,2, Ramou Njie1,2
&Corresponding author
Amoebic liver abscess is common in low middle income countries and is mostly associated with poor sanitary condition. There is limited data describing patients with cardiac tamponade and right pleural effusion secondary to amoebic liver abscess in resource limited settings. We describe a 16-year-old female, grade 9 student who was diagnosed with cardiac tamponade and right pleural effusion secondary to amoebic liver abscess. Patient was successfully managed with metronidazole and repeated ultrasound guided-percutaneous needle aspiration. Chest X-ray was used in monitoring the patient�s progression. In resource limited settings, where there are no pigtail catheters or trained cardiac surgeons, early diagnosis with prompt initiation of metronidazole and repeated ultrasound guided-percutaneous needle aspiration of the liver abscess may help treat and prevent complications in these patients.

Amoebic liver abscess (ALA) is common in low middle income countries and is mostly associated with poor sanitary condition [1]. Complications such as peritonitis, pleural, pericardial or brain disease may occur due to rupture of the liver abscess, direct extension or through haematogenous spread. These complications occurs in less than 2% of patients who have ALA in the left lobe of the liver [2,3]. Patients with pericardial amoebic disease usually present with fever, chest pain, and progressive dyspnea and can eventually progress to cardiac tamponade [3]. Case reports describing patients with cardiac tamponade and pleural effusion secondary to ALA are very rare. We present a 16-year-old female, who was diagnosed with cardiac tamponade and right pleural effusion secondary to ALA. Patient was successfully managed with metronidazole and repeated ultrasound guided-percutaneous needle aspiration.

Patient information: a 16-year-old female, grade 9 students, referred from a tertiary hospital where she was admitted for 5 days. She presented with a 4-week history of abdominal pain and distension. This was associated with non-bloody, non-mucoid stools, chest pain and fever. She had no significant past medical history.
Clinical findings: on examination, she was acutely ill looking, in respiratory distress, pale (+), anicteric, with pedal oedema (+). Abdomen was distended with a smooth, tender hepatomegaly. The percussion nodes were stony dull in the right lower lung field with reduce intensity of the breath sounds. The heart sounds were also heard but distant. Vital signs showed blood pressure of 95/75 mmhg, pulse rate of 140 beats/minute, respiratory rate of 38 cycles/minute, and temperature: 37.3°C.
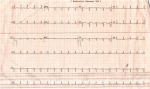
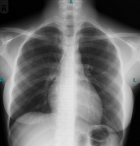
Diagnostic assessment: investigations showed a negative hepatitis B surface antigen, hepatitis C virus antibody and Human immunodeficiency virus tests. Her full blood count, Liver function tests, erythrocyte sedimentation rate results at presentation are shown in Table 1. Stool microscopy was negative for ova or cyst and culture didn´t yield any growth. Initial abdominal scan by a radiology technician showed an enlarged liver and contains a huge mass measuring >10 x 8.4 cm with dense fluid collection in the left lobe of the liver suggestive of a liver abscess (Figure 1). Blood culture also didn´t grow any organism. Microscopy and culture of the aspirate from the abscess didn´t yield any organism. Gene x pert for mycobacterium tuberculosis was also not detected. Chest X-ray at presentation showed cardiomegaly and right pleural effusion (Figure 2). Electrocardiography also showed sinus tachycardia with low voltages in all leads (Figure 3). Bedside echocardiography also showed pericardial effusion predorminant around the left ventricle (2.1cm) and lowest in the apical area (0.7cm).
Diagnosis: all the above clinical, laboratory and imaging results confirmed the diagnosis of cardiac tamponade and pleural effusion secondary to ALA.
Therapeutic interventions: she was admitted and put on IV ciprofloxacillin 500mg twice daily (BD) and metronidazole 800mg three times a day (TDS) for 3 weeks. Oral metronidazole 800mg TDS was continued for 1 week. Percutaneous ultrasound-guided needle aspiration of the liver abscess was done by the clinician on 3 different occasions and 1.575 litres (550mls, 625 mls and 400mls respectively) of odourless, brownish paste like pus was drained (Figure 4).
Follow up and outcome of interventions: at discharge 3 weeks after presentation, patient was much better and had no complains. Chest X-ray (Figure 5) 4 months after admission, liver function tests and full blood count results done at discharge and 4 months after admission respectively showed improvement (Table 1). The patient was then discharged from the clinic and has been asymptomatic for the past 3 years.
This case report describes a patient who was diagnosed with cardiac tamponade and right pleural effusion secondary to ALA. She was treated with metronidazole and repeated ultrasound guided-percutaneous needle aspiration of the liver abscess. Amoebic liver abscess is an extra-intestinal manifestation of amoebiasis and is caused by the protozoan entamoeba histolytica that migrates from the intestine to the liver via the portal vein. It is common in low middle income countries and is mostly associated with poor sanitary conditions [3,4]. Amoebic liver abscess is common amongst males than females and mostly occur between the 18-50 years age [2]. Our patient is a 16-year-old female from a low socioeconomic background who presented with gastroenteritis.
Complications such as peritonitis, pleural, pericardial or brain disease may occur due to rupture of the liver abscess, direct extension or through haematogenous spread. Pleuropulmonary complications are the most common, followed by intraperitoneal rupture of abscess in incidence. Pericardial and cerebral amoebiasis are relatively rarer complications [3]. If pericardial amoebiasis is not treated early, it can lead to cardiac tamponade and subsequent death. In our report, we describe a case of a liver abscess in the left lobe of the liver that resulted in both pleuropulmonary and pericardial complications. The patient also developed cardiac tamponade due to the massive pericardial effusion at the time of presentation. The presence of an abscess in the left lobe with associated cardiac tamponade and right pleural effusion as in our case is rare; however, with timely diagnosis and treatment, a fatal outcome can be prevented. The diagnosis of cardiac tamponade includes both clinical and investigations, such as electrocardiography, echocardiography and chest X-ray [5,6]. Our patient presented with chest pain, shortness of breath, tachycardia, hypotension and muffled heart sounds which are typical clinical manifestations. Electrocardiography also showed sinus tachycardia with low QRS complexes in all leads, echocardiography also revealed pericardial effusion with compression of the right ventricle and chest X-ray showed a massive cardiomegaly. All these findings confirm the diagnosis of cardiac tamponade in our patient. Another important finding on echocardiography was the presence of fibrin strands which may mimic pericarditis due to tuberculosis. It is thus important to include amoebic pericarditis as a differential diagnosis in patients with this echocardiography finding.
As already reported in other cases, pericardial effusion due to amoebic liver abscess are managed with percutaneoues pericardiocentesis [7-9] or subxiphoid percutaneous pig tail catheters or cardiac surgery [2]. In our case, the patient was put on metronidazole and the liver abscess was repeated drained by ultrasound guided-percutaneous needle aspiration which resulted in complete resolution of both the pericardial and pleural effusion. The resolution of the pericardial and pleural effusion was monitored using repeated chest X-rays. In resource limited settings, where there are no pigtail catheters or trained cardiac surgeons, early diagnosis with prompt initiation of metronidazole and repeated ultrasound guided-percutaneous needle aspiration of the liver abscess may help treat these patients.
Cardiac tamponade and right pleural effusion secondary to left lobe ALA is a rare and fatal complication. In resource limited settings, where there are no pigtail catheters or trained cardiac surgeons, early diagnosis with prompt initiation of metronidazole and repeated ultrasound guided-percutaneous needle aspiration of the liver abscess may help treat and prevent complications in these patients.
The authors declare no competing interests.
Sheikh Omar Bittaye, Saydiba Tamba and Ramou Njie conceived the case report and did the data collection. Sheikh Omar Bittaye and Saydiba Tamba did the percutaneous drainage. All authors contributed to the drafting and revision of the manuscript. All authors read and approved the final version of the manuscript.
Table 1: laboratory investigations at presentation, at discharge and 4 months after presentation
Figure 1: ultrasound scan showing a huge hypoechoic mass in the liver
Figure 2 chest X-ray at the time of presentation
Figure 3 electrocardiography at admission show low voltages in all leads and tachycardia
Figure 4 brown, odorless, thick paste-like pus drained from the liver abscess
Figure 5 chest X-ray 4 months after admission
- Khim G, Em S, Mo S, Townell N. Liver abscess: Diagnostic and management issues found in the low resource setting. Br Med Bull. 2019 Dec 11;132(1):45-52. PubMed | Google Scholar
- Francis C, Soni S, Gupta A, Agstam S. A case report of ruptured amoebic liver abscess causing cardiac tamponade and requiring pericardial window. Eur Heart J Case Rep. 2020 Aug 30;4(5):1-4. PubMed | Google Scholar
- Raza M, Kumar S, Nanjiani D, Hussain A, Azizullah S. Pericardial Effusion Secondary to Amoebic Liver Abscess: A Rare Complication. 2020;12(11):5-12. PubMed | Google Scholar
- Anasi AJ, Gluckman S. Amebic Liver Abscess. Clin Liver Dis (Hoboken). 2015 Aug 24;6(2):41-43. PubMed
- Ball JB, Morrison WL. Cardiac tamponade. Postgrad Med J. 1997 Mar;73(857):141-5. PubMed
- Ang KP, Nordin RB, Lim SCY, Lee CY, Lu HT. Diagnostic value of electrocardiogram in cardiac tamponade. Med J Malaysia. 2019;74(1):51-6. PubMed | Google Scholar
- Adeyemo AO, Aderounmu A. Intrathoracic complications of amoebic liver abscess. J R Soc Med. 1984 Jan;77(1):17-21. PubMed | Google Scholar
- Bansal BC, Gupta D. Amoebic Pericarditis. Postgrad Med J. 1971 Oct;47(552):678-80. PubMed | Google Scholar
- Baid CS, Varma AR, Lakhotia MA. A case of subacute effusive constrictive pericarditis with a probable amoebic aetiology. Br Heart J. 1987 Sep;58(3):296-8. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures



Article metrics

