
Marburg variant of multiple sclerosis masquerading as glioma: a case report
Campbell Chukwuebuka Francis, Adegboye Michael Olakunle, Oti Bibiana, Ajare Enyereibe Chuks, Hart Idawarifagha, Okwunodulu Okwuoma, Ndubuisi Anele Chika, Ohaegbulam Chukwunonyerem Samuel
Corresponding author: Campbell Chukwuebuka Francis, Department of Neurosurgery, Memfys Hospital, Enugu, Nigeria 
Received: 07 Jul 2022 - Accepted: 03 Jan 2023 - Published: 12 Jan 2023
Domain: Neurology (general)
Keywords: Demyelination, Marburg, multiple sclerosis, tumefactive necrosis, case report
©Campbell Chukwuebuka Francis et al. PAMJ Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Campbell Chukwuebuka Francis et al. Marburg variant of multiple sclerosis masquerading as glioma: a case report. PAMJ Clinical Medicine. 2023;11:16. [doi: 10.11604/pamj-cm.2023.11.16.36244]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com//content/article/11/16/full
Case report 

Marburg variant of multiple sclerosis masquerading as glioma: a case report
Marburg variant of multiple sclerosis masquerading as glioma: a case report
![]() Campbell Chukwuebuka Francis1,&, Adegboye Michael Olakunle1, Oti Bibiana2, Ajare Enyereibe Chuks3, Hart Idawarifagha1, Okwunodulu Okwuoma1, Ndubuisi Anele Chika1, Ohaegbulam Chukwunonyerem Samuel1
Campbell Chukwuebuka Francis1,&, Adegboye Michael Olakunle1, Oti Bibiana2, Ajare Enyereibe Chuks3, Hart Idawarifagha1, Okwunodulu Okwuoma1, Ndubuisi Anele Chika1, Ohaegbulam Chukwunonyerem Samuel1
&Corresponding author
Marburg variant of multiple sclerosis is a rare demyelinating disease with a rapid and often fulminant course. It may disguise as a cerebral ring-enhancing lesion, hence presenting a diagnostic dilemma. Treatment may be challenging due to its rarity, aggressive course and dearth of diagnostic facilities in our environment. To the authors' best knowledge, this is the first reported case of the Marburg variant of multiple sclerosis in sub-Saharan Africa. We present a 35-year-old woman with clinical and radiological features of intracranial space-occupying lesion who had two recurrences over four months despite total gross resections. The fulminant, recurrent nature of this disease, coupled with positive oligoclonal bands, led to the Marburg variant of multiple sclerosis diagnosis. Physicians saddled with managing neurological diseases should consider this a differential diagnosis, especially when the clinical course and laboratory findings have ruled out more common neoplastic and infective causes.

Marburg disease (MD) is a rare variant of multiple sclerosis (MS) characterized by acute severe demyelination of white matter tracts and an aggressive clinical course that may progress to severe disability or death within weeks to months [1,2]. Otto Marburg first described it in 1906 after noting its aggressive nature in three patients, distinct from other forms of MS [3]. The hallmark of the disease is the multifocal or diffuse neuro-inflammatory reaction with predominant macrophage and lymphocyte infiltration resulting in extensive axonal destruction, accumulation of demyelinating plaques and cavitations. Cerebralspinal fluid (CSF) analysis may show pleocytosis, elevated protein, high immunoglobulin G and positive oligoclonal bands [4,5].
The subcortical and brainstem demyelinating plaques usually present with a mass effect that mimics infective and neoplastic intracranial space-occupying lesion (ICSOL) commonly seen in our sub-region and may cause a diagnostic dilemma for the managing physician [1,2]. The diagnosis of MD is based on the rapid fulminant clinical course and neuroimaging finding suggestive of a demyelinating mass lesion and the presence of an oligoclonal band in CSF.
We present a young lady with rapid and progressively worsening neurological deficit due to a right frontoparietal space-occupying lesion that recurred twice in four months despite gross total resections and immunosuppressive therapy. We diagnosed Marburg disease based on the fulminant clinical course, rapid, relentless recurrence, histological feature of inflammatory demyelinating plaques and positive oligoclonal bands in CSF. There is a paucity of reports of multiple sclerosis in sub-Saharan Africa, more so for the Marburg variant, unlike in western literature [1,3,5-8].

Patient information: we present a 35-year-old right-handed woman with a three-month history of headaches, left hemibody weakness and painless progressive bilateral visual impairment culminating in visual loss a week prior to presentation. There were also histories of generalized tonic-clonic seizures, personality changes and associated alteration in the sensorium three days before presentation. She had no features suggestive of intracranial infections, systemic tuberculosis, metastatic disease, or a family history of similar illness. There was a long referral chain before she presented to our facility.
Clinical findings: physical examination revealed a young woman with a Glasgow coma score (GCS) of 13, which dropped to 9 (E2V3M4) while in the emergency room. She had no light perception in both eyes, and fundoscopy revealed bilateral pale atrophic discs with blurred margins. There was spastic left hemiparesis but no sensory deficits.
Timeline of the current episode: symptoms had an initial insidious onset characterized by headaches and left hemibody weakness but rapidly progressed to visual impairment and alteration in sensorium a week prior to presentation.
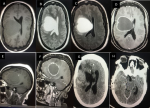
Diagnostic assessment and therapeutic interventions: brain magnetic resonance imaging (MRI) (Figure 1(A-F)) showed a right frontoparietal ring-enhancing mass lesion with the ring open towards the ventricle. Laboratory work-up, including inflammatory markers, were normal (CRP- 8.37 mg/L, ESR- 45mm/hr). Based on the above findings, we diagnosed a right frontoparietal abscess with high-grade glioma and tuberculoma as differential diagnoses.
She had an emergency craniotomy and excision of the mass lesion. The decision for surgery was due to the sudden worsening of her clinical condition with a drop in GCS. The intraoperative finding was a cyst-like cavity containing brownish fluid with a surrounding area of gliosis. Initial histology was not helpful as it revealed a haemorrhagic cyst of nonspecific origin. The postoperative brain computed tomography (CT) scan revealed no residual lesion (Figure 1(G,H)). Culture of the cystic fluid yielded no growth. Fungal studies and GeneXpert MTP/RIF test were all negative. CSF analysis revealed elevated CSF albumin, IgG and IgG index, and the oligoclonal bands was positive. These findings suggested a diagnosis of tumefactive multiple sclerosis. She was commenced on high-dose steroids (intravenous methylprednisolone one gram daily for five days and tapered to oral maintenance dose). She made good neurological improvement; GCS improved to 15 with the resolution of irrational talk and improvement in the left hemiparesis however, visual impairment persisted. Oral azathioprine was added to her medications, and she was discharged after about six weeks of admission with a modified rankin score (mRS) of 2.
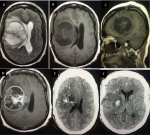
She, however, represented to the emergency room four weeks after discharge unconscious, with recurrent seizures, headaches worse in the morning, nausea, recurrent vomiting and worsening hemiparesis. The post-resuscitation GCS was 9 (E2V2M5). Repeat brain MRI showed recurrence of the mass lesion with a similar ring-enhancing pattern and significant perilesional oedema with subfalcine and uncal herniations (Figure 2(A-D)). This recurrence occurred despite being on oral immunosuppressives. A decision was taken to urgently relieve the intracranial pressure by releasing the previous craniotomy. The intra-operative finding was a cystic mass containing dirty brown fluid with a surrounding area of gliosis. No purulent material or obvious mass lesion was seen. The postoperative brain CT scan revealed no evidence of residual lesion except for minimal operative bed haematoma (Figure 2(E,F)). Again, all microbiological cultures and immunohistochemistry yielded no organism. Microscopy section showed an acute demyelinating inflammatory brain lesion with many macrophages imbibing lipid-like myelin materials with some lymphocytes surrounding blood vessels as well as areas of inflammation (no overt neoplasm was seen) (Figure 3).
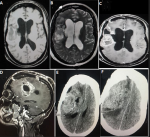
Follow-up and outcome: she made significant improvement post-operatively; GCS improved to 15 but was still hemiparetic and had no light perception in both eyes. Upon histologic confirmation of a demyelinating lesion, the clinical course of the disease and the CSF findings, a diagnosis of tumefactive multiple sclerosis, likely the Marburg variant, was made. She had a repeat (second) 5-day course of high dose methylprednisolone (1 gram daily for five days) and subsequently intravenous cyclophosphamide 500mg weekly for five weeks and was later placed on maintenance steroids. After the fourth course of cyclophosphamide, she had a repeat brain MRI (Figure 4(A-C)) and CT a month later (Figure 4(D,E)), which revealed yet another recurrence (the second recurrence in four months). The disease progression continued despite medications. Monoclonal antibodies were not available, and the patient could not afford plasmapheresis. She succumbed to the illness about ten months after the diagnosis.
Patient perspective: she believed that there was a spiritual aspect of her illness that triggered the persistent recurrence. Unfortunately, she passed on despite all interventions.
Informed consent: the patient�s relatives gave informed consent for the publication of this article.
Marburg disease (MD) is often described as a malignant form of multiple sclerosis characterized by severe and progressive demyelinating encephalitis [1,2,4,5]. It results in massive neuronal destruction and extensive axonal injury, causing significant neurologic impairment and severe disability or death, usually within a year. The hallmark of the disease is relentless progression and recurrences despite high-dose immunosuppressive and anti-inflammatory agents [5-8]. Our index patient had a profound neurologic disability that progressed rapidly to blindness, hemiparesis, speech deficit and cognitive decline within three months of diagnosis and recurred twice within four months despite maximum surgical resection and use of immunosuppressive agents. This is typically seen in the Marburg variant of multiple sclerosis [6].
Diagnosis is made based on the appropriate clinical picture, presence of oligoclonal bands in CSF and histology showing acute demyelination [1,5,6]. We found a highly destructive lesion with extensive macrophage and T-cells infiltration on histology, with the macrophages engulfing myelin breakdown products and associated cavitations and overt necrosis. There were no neoplastic cells or purulent materials, which excludes malignant or infective causes. Marburg disease (MD) usually has tumefactive features mimicking intracranial SOL [1,3,5]. The massive demyelinating plaques are often centred deep in the white matter and have MRI features similar to other infective and neoplastic masses. The enhancement pattern post gadolinium administration is usually a ring mass which is nonspecific. Most authors agree that extensive surgery is unnecessary in demyelinating lesions and recommend minimal access biopsy instead [3,6]. However, we chose urgent surgical decompression because of the lesion size in the index patient, the mass effect causing herniation syndrome and rapid neurological deterioration. In the face of diagnostic uncertainty, especially in developing countries where challenges of health care financing exist and common ring-enhancing lesions like glioblastoma, toxoplasmosis, intracranial abscess, and tuberculoma are prevalent, open decompression tends to serve both therapeutic and diagnostic purposes [9,10].
Neuromyelitis Optica (NMO) is a close differential because she had blindness as an early presenting symptom. However, NMO rarely occurs with tumefactive brain lesions, and CSF oligoclonal bands are usually negative [5,11]. Furthermore, she did not have clinical features suggestive of transverse myelitis typically seen in NMO. We lack facilities for aquaporin-4 assessment, but the clinical picture, the MRI findings, and the steroid-resistant nature makes the diagnosis of NMO unlikely [11]. Another consideration was acute demyelinating encephalomyelitis (ADEM) which presents with rapid demyelination often preceded by a febrile illness or vaccination [5,12]. Imaging in ADEM also displays tumefactive lesions in selected cases; however, they are often multiple and have indistinct borders as compared with the smooth enhancement noted in our patient. In addition, ADEM is seen more often in the paediatric population and is often monophasic with an excellent response to steroid therapy, unlike MD, which often lacks prodromal illness, is seen more in adult females and is generally resistant to steroid administration [12].
The worrisome problem noted in her management was her repeated recurrences within four months despite completing two pulse courses of high-dose methylprednisolone and low-dose cyclophosphamide. This resistance pattern has been widely reported in the literature in patients with the Marburg variant of MS [1,2,5,6]. Treatment recommendations vary from high-dose cyclophosphamide, mitoxantrone, rituximab, immunoglobulin G and plasmapheresis with varying results [1,5,6,8,12]. However, most of these other treatment options are either unavailable in our environment or overwhelmingly expensive.
Although MD and other tumefactive MS lesions are uncommon in developing countries, they can pose significant diagnostic dilemmas and management challenges to surgeons in the sub-region as they are the possible differential diagnoses of intracranial SOL [13]. Furthermore, the scarcity and the high cost of these essential neuroimaging facilities in our society compounds the situation. Though Marburg disease generally has poor outcomes as reported in the literature, late presentation, poverty, ignorance and lack of expertise make diagnosis challenging and the outcome grim for patients within our sub-region.
Marburg disease is a variant of MS characterized by an aggressive and fulminant clinical course often resistant to immunosuppressives. The unavailability of advanced diagnostic facilities and a narrow range of treatment options compounds management in our resource-poor setting. This should be considered a differential diagnosis by physicians, especially when the clinical course and laboratory findings have ruled out more common neoplastic and infective causes of such a mass lesion.
The authors declare no competing interests.
Adegboye Michael Olakunle, Campbell Chukwuebuka Francis, Oti Bibiana, Ndubuisi Anele Chika, Okwunodulu Okwuoma, Ndubuisi Anele Chika and Ohaegbulam Chukwunonyerem Samuel were involved in writing up the manuscript; Campbell Chukwuebuka Francis and Ajare Enyereibe Chuks were involved in reviewing the images. All the authors involved in patient management read and approved the final version of this manuscript.
The authors acknowledge the cooperation they got from the patient and relatives.
Figure 1: preoperative (first surgery) brain MRI; (A-F) axial and sagittal brain MRI images showing right frontoparietal well-circumscribed T1 isointense mass lesion with associated effacement of ipsilateral lateral ventricle and midline shift, the mass is hyperintense on T2 and has ring enhancement post contrast with open end towards the ventricle, suggestive of cerebral abscess; (G,H) post-operative axial non contrast brain CT images and postoperative CT showing gross total resection of the mass
Figure 2: brain MRI after first recurrence (A-D); axial and sagittal brain MRI images showing right frontoparietal T1 hypointense mass lesion with evidence of mass effect, the mass is hyperintense on T2 and has cortical based open ring post contrast administration, this suggests tumefactive multiple sclerosis; (E,F) post-operative axial non contrast brain CT images and postoperative brain CT scan after second surgery showing minimal haematoma at the operation site but no evidence of residual mass lesion
Figure 3: (A) inflammatory changes; (B) macrophage destruction of myelin with cystic changes in the brain lesion
Figure 4: axial brain MRI images; (A,B) right frontoparietal T1 and T2 mixed intense but predominantly hypointense mass lesion; (C,D) post-contrast image showing peripheral enhancement; (E,F) contrast CT images taken a month later displaying the recurring mass lesion, this is the second recurrence within four months
- Nozaki K, Abou-Fayssal N. High dose cyclophosphamide treatment in Marburg variant multiple sclerosis A case report. J Neurol Sci. 2010 Sep 15;296(1-2):121-3. PubMed | Google Scholar
- Johnson MD, Lavin P, Whetsell WO Jr. Fulminant monophasic multiple sclerosis, Marburg's type. J Neurol Neurosurg Psychiatry. 1990;53(10):918-21. PubMed | Google Scholar
- Capello E, Mancardi GL. Marburg type and Balò's concentric sclerosis: rare and acute variants of multiple sclerosis. Neurol Sci. 2004;25:361-3. PubMed | Google Scholar
- Ludwig A, Duvall J, Peterson JE, Hakimi R. Marburg�s Variant of Multiple Sclerosis with Extensive Brain Lesions: An Autopsy Case Report. J Neurol Neurother. 2015;2(1):8-11. Google Scholar
- Suzuki M, Kawasaki H, Masaki K, Suzuki SO, Terada T, Tsuchida T et al. An autopsy case of the Marburg variant of multiple sclerosis (acute multiple sclerosis). Intern Med. 2013;52(16):1825-32. PubMed | Google Scholar
- Avila-Ornelas J, Labat E, Alfonso G, Serrano C, Fiorito F. An extremely aggressive case of Marburgs disease treated with high dose cyclophosphamide. A case report. Mult Scler Relat Disord. 2019;31:51-3. PubMed | Google Scholar
- Manuel A, Vasudevan MC. A Case of Marburg's Variant of Multiple Sclerosis Successfully Treated with IVIg and Mitoxantrone. Ann Indian Acad Neurol. 2021 Jan-Feb;24(1):92-94. PubMed | Google Scholar
- Jeffery DR, Lefkowitz DS, Crittenden JP. Treatment of Marburg variant multiple sclerosis with mitoxantrone. J Neuroimaging. 2004;14(1):58-62. PubMed | Google Scholar
- Santosh V, Mahadevan A, Chickabasaviah TY, Bharath RG, Krishna SS. Infectious lesions mimicking central nervous system neoplasm. Semin Diagn Pathol. 2010;27(2):122-35. PubMed | Google Scholar
- Ndubuisi CA, Ndukuba KO, Okwuoma OO, Iroegbu LU, Ohaegbulam SC. Dominant hemisphere and upper cervical cord tumefactive multiple sclerosis in a Nigerian teenager initially misdiagnosed and managed. Orient Journal of Medicine. 2019 May 31;31(1-2):61-6. Google Scholar
- Jarius S, Wildemann B, Paul F. Neuromyelitis optica: clinical features, immunopathogenesis and treatment. Clin Exp Immunol. 2014 May;176(2):149-64. PubMed | Google Scholar
- Elenein RG, Sharer LR, Cook SD, Pachner AR, Michaels J, Hillen ME. A second case of Marburg's variant of multiple sclerosis with vasculitis and extensive demyelination. Mult Scler. 2011;17(12):1531-8. PubMed | Google Scholar
- Campbell FC, Oti B, Ndafia NM, Hart I, Okwunodulu O, Ndubuisi CA et al. Balo's concentric sclerosis a rare variant of multiple sclerosis in a Nigerian adult male: A case report. Surg Neurol Int. 2022;13:486. Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures

Article metrics

