
Isolated medial malleolar non-union, a cancellous screw with Kirshner wire as a valid and practical option: a case report
Sergio Candido Ekekang Ncogo Nsegue, Hamza Berrada, Paul Koulemou, Bennis Azzelarab, Salim Bouabid
Corresponding author: Sergio Candido Ekekang Ncogo Nsegue, Department of Traumatology and Orthopedic Surgery, Mohammed V Military University Hospital, Rabat, Morocco 
Received: 26 Dec 2022 - Accepted: 05 Feb 2023 - Published: 07 Feb 2023
Domain: Orthopedic surgery,Surgical Sciences
Keywords: Medial malleolus, non-union, bone graft, case report
©Sergio Candido Ekekang Ncogo Nsegue et al. PAMJ Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Sergio Candido Ekekang Ncogo Nsegue et al. Isolated medial malleolar non-union, a cancellous screw with Kirshner wire as a valid and practical option: a case report. PAMJ Clinical Medicine. 2023;11:34. [doi: 10.11604/pamj-cm.2023.11.34.38648]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com//content/article/11/34/full
Case report 

Isolated medial malleolar non-union, a cancellous screw with Kirshner wire as a valid and practical option: a case report
Isolated medial malleolar non-union, a cancellous screw with Kirshner wire as a valid and practical option: a case report
![]() Sergio Candido Ekekang Ncogo Nsegue1,&, Hamza Berrada1, Paul Koulemou1, Azzelarab Bennis1, Salim Bouabid1
Sergio Candido Ekekang Ncogo Nsegue1,&, Hamza Berrada1, Paul Koulemou1, Azzelarab Bennis1, Salim Bouabid1
&Corresponding author
Medial malleolar fracture non-union are relatively uncommon. Not many studies have been found in the literature concerning its management, the great majority of studies in the orthopedic literature describe the use of either two cancellous screws or tension band wiring for its management. The use of one cancellous screw with Kirshner wire has not been described in the literature for the management of medial malleolar non-union. In this article we present two cases of medial malleolus non-union successfully managed with a sole cancellous screw associated with a Kirshner wire in two patients highlighting its possible advantages and a review of the literature on the management of medial malleolar non-union.

There are few focused reviews on the management of non-union of isolated medial malleolar ankle fractures. Even though non-union of medial malleolus fracture is rare, it accounts for about 5-30% of all medial malleolar fractures which leads to long term complications like pain causing disabilities, instability and inflammation that needs an active intervention for a permanent relief [1]. For their management, most studies have described the use of either two compression screws with adjuvant bone graft [2] or tension band wiring with adjuvant bone graft [3]. To our knowledge, there has been no description of the use of a sole cancellous screw associated with a Kirshner wire with adjuvant bone graft for the management of medial malleolus nonunion, which we describe and which gave very satisfactory clinical outcomes.

Patient 1
Patient information: a 30-year-old non-diabetic and non-smoker male that worked as a public transport driver presented to us complaining of a persistent pain of the right ankle which had been going on for 6 years and had been increasing progressively leaving him with an antalgic gait when walking, although the symptoms were mild at rest. The patient reported being involved in a motor accident 6 years earlier leaving him with some pain in his right ankle and with some auto medication and some rest he felt better and neglected the pain then went on with his activities.
Clinical findings: our examination revealed pain on the palpation of the medial malleolus and motion of the ankle from dorsiflexion to neutral position. Neurologic and vascular examination of the affected limb were normal.
Timeline of current episode: the patient reported being involved in a motor accident, leaving him with some pain in his right ankle 6 years before he was presented to us.
Diagnostic assessment: plain radiographs and CT scans were performed, which revealed the diagnosis of medial malleolar atrophic nonunion without any associated lateral lesion (Figure 1 (A,B,C,D).
Diagnosis: all the above clinical and imaging results confirmed the diagnosis of medial malleolar atrophic nonunion without any associated lateral lesion.
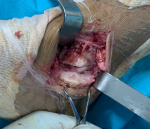
Therapeutic interventions: surgery was decided for its management. Under regional epidural anesthesia, the patient was placed in a supine position and a tourniquet was used. The standard medial approach was used, centered at the medial malleolus, and the incision was anteriorly curved distally. The fragment was identified, and the fracture site exposed (Figure 2). The fracture site was cleared of debris, including periosteal remnants and fibrous tissue revealing a relatively small sized malleolar fragment with sclerotic bone, the fracture ends were freshened until punctate bleeding was observed (Figure 3). The fracture gap was then filled with cancellous bone graft from the ipsilateral iliac crest. The fracture was then reduced using a pointed reduction clamp under intraoperative C-arm imaging and fixed with two parallel 2�mm K-wires with purchase at the lateral cortex of the tibia (Figure 4 A). One Kirshner wire was then replaced with a 3.5�mm partially threaded cancellous screw. An additional 2�mm K-wire was introduced from medial to lateral above the fracture line to fix a cortical fragment that risked detachment, this wire was directed anteriorly so as not to interfere with the syndesmosis (Figure 4 B,C). The ankle was immobilized in a below-knee slab for 4 weeks, followed by gradual ankle range of motion (ROM) exercises. The patient was kept non-weight-bearing for 6 weeks, and then partial weight-bearing in a protective boot, the K-wires were removed at 8 weeks during a regular follow-up day.
Follow-up and outcome of interventions: the patient had an excellent recovery with no pain and very good functional outcome after 8 months follow up.
Patient perspective: “It has been 8 months since surgery and I can finally walk again with very little discomfort as opposed to the years following my accident”
Informed consent: the patient gave an informed written consent about the publication of this article.
Patient 2
Patient information: a 27-year-old farmer, non-diabetic and non-smoker presented to us complaining of a persistent right ankle pain which had been going on for one year after a fall from a tree. He reported having consulted another center after the fall, and he was given some pain medication and rest, but the symptoms kept increasing which prompted him to seek medical attention at our center.
Clinical findings: the palpation of the medial malleolus revealed pain. Ankle range of motion was reduced due to pain.
Timeline of current episode: ankle pain had been going on for a year before the patient was addressed to us.
Diagnostic assessment: plain radiographs of the ankle revealed an atrophic nonunion of the medial malleolus (Figure 5 A,B).
Diagnosis: all the above clinical and imaging results confirmed the diagnosis of medial malleolar atrophic nonunion without any associated lateral lesion.
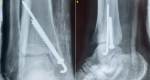
Therapeutic interventions: the patient was operated using the same technique as described above without a third K-wire needed. The fracture was fixed using a 2�mm K-wire with a purchase at the lateral tibial cortex and a 4.5 partially threaded cancellous screw after cancellous bone grafting from the ipsilateral iliac crest (Figure 6 A,B). The ankle was immobilized in a below-knee slab for 4 weeks, followed by gradual ankle range of motion (ROM) exercises. The patient was kept non-weight-bearing for 6 weeks, and then partial weight-bearing in a protective boot, the K-wire was removed at 6 weeks during a regular follow-up day.
Follow-up and outcome of interventions: the patient had an excellent recovery with no pain and very good functional outcome after 8 months follow up.
Patient perspective: “I feel much better with a painless ankle when walking”
Informed consent: the patient gave informed written consent about the publication of this article.
There is an abundance of literature about fracture nonunion, but the literature is very limited on the topic of unhealed medial malleolus fractures. Studies confirm the rate of nonunion for acute fractures of the medial malleolus treated conservatively to be as high as 10% to 15% [4]. Local and systemic reasons which predispose a fracture to nonunion are generally well understood. Systemic factors include diabetes mellitus, smoking, alcohol use, obesity, advanced age, and radiation therapy. Watson and jones attributed the non-union of medial malleolus to the three following factors: (a) feeble osteogenic activity, (b) obliteration of the fracture hematoma by collapse of the surrounding soft tissues, and (c) interposition of a flap of periosteum and other soft tissues [5]. Indications for surgical fixation of medial malleolus nonunion include significant pain and a consequential antalgic gait, tibialis posterior tenosynovitis, and/or ankle instability [6]. The most commonly employed technique to fix symptomatic medial malleolar nonunion is a fixation comprised of two screws. Khurana et al. [7] reported three cases of medial malleolus nonunion in their mixed cohort study of 15 bimalleolar nonunion, one patient underwent fixation using two screws and the other using a plate and screws. Both patients also underwent augmentations with iliac crest aspirate (ICA), bone morphogenic protein (BMP)-7 and BMP cancellous chips. The third patient underwent a medial malleolus resection. They reported good functional outcomes in all cases.
Mahdu et al. [2] describes a series of three medial malleolar non-unions treated with two parallel partially threaded cancellous screws with purchase of the lateral tibial cortex associated with bone graft. They report satisfactory results, highlighting the importance of a purchase of the lateral tibial cortex for better stability of the fixation of these fractures. The purchase of the lateral tibial cortex was obtained by the Kirchner wire in our two cases. Tension band wiring has also been reported as a means of management of medial malleolus fracture non-union in recent literature by John Rakesh et al. [3] and Tanna et al. [8]. They both describe treating one patient each with tension band wiring using tricortical bone graft, with good results after follow up. Both our patients had excellent recovery with no pain and very good functional outcome after 8 months follow up. The use of a single screw associated with a k-wire will have the benefits of screw compression. Good lateral tibial cortex purchase with the k-wire. Less destruction of the graft as opposed to the use of two screws. In the case of tension band wiring lesser periosteal stripping during surgery, and removal of hardware can be done by small stab incision with local anesthetic. Less cost also for the patient due to the use of cheaper implants compared to the use of two screws and no second surgery as compared to tension band wiring for implant removal. Small fragments which do contribute to ankle stability do have to be fixed, the use of two screws in these cases can be difficult or impossible due to the size of the fragment and the high risk of splitting the fragment, in these cases a single screw for compression associated with a k-wire is a valid option.
Isolated medial malleolar fracture nonunion are relatively uncommon. Various methods of treatment have been described in the literature. The use of a sole cancellous screw and k-wires associated with bone grafting yields very good results and has its advantages, especially when treating with small malleolar fragments while giving good compression as well as providing rotational stability.
The authors declare no competing interests.
Data collection: Sergio Candido Ekekang Ncogo Nsegue, Paul Koulemou and Hamza Berrada. Written manuscript: Sergio Candido Ekekang Ncogo Nsegue. Conception, Interpretation and Intellectual content: Sergio Candido Ekekang Ncogo Nsegue and Azzelarab Bennis. Intellectual content of critical importance and article review: Azzelarab Bennis and Salim Bouabid. All authors read and approved the final manuscript.
Figure 1: (A,B,C,D) CT scans and plain radiographs of the ankle revealing the medial maleolar non-union
Figure 2: non-union fracture site exposed with debris and fibrous tissue
Figure 3: fracture site freshened
Figure 4: (A) fracture fixed with two parallel 2mm K-wires; (B) definitive fixation after replacing one Kirshner wire with a 3.5mm partially threaded cancellous screw and additional anterior Kirshner wire to fix a loose medial cortical fragment; (C) lateral fluoroscopic view of definitive fixation
Figure 5: (A, B) plain radiographs showing medial malleolus non-union
Figure 6: (A,B) definitive fixation with ankle in a below knee slab
- Herscovici D, Scaduto JM, Infante A. Conservative treatment of isolated fractures of the medial malleolus. J Bone Joint Surg Br. 2007;89(1):89-93. PubMed | Google Scholar
- Madhu T, Morgan-Jones R. A modified operative technique for enhanced compression of medial malleolar non-union. Injury Extra. 2005;36:520-525. Google Scholar
- John R, Dhillon MS, Khurana A, Aggarwal S, Kumar P. Tension Band Wiring Is As Effective As A Compression Screw In A Neglected, Medial Maleolus Non-Union: A Case-Based Discussion & Literature Review. J Orthop Case Rep. 2017 Jul-Aug;7(4):72-75. PubMed | Google Scholar
- Reider B, Falconiero R, Yurkofsky J. Nonunion of a medial malleolus stress fracture: A case report. The American Journal of Sports Medicine. 1993;21(3):478-481. PubMed | Google Scholar
- Watson-Jones SR. Fractures and joint injuries. 4 th ed. Baltimore: William and Wilkins; 1957.
- Banks SW. The treatment of non-union of fractures of the medial malleolus. J Bone Joint Surg Am. 1949;31A(3):658-662. PubMed | Google Scholar
- Khurana S, Karia R, Egol KA. Operative treatment of non-union following distal fibula and medial malleolar ankle fractures. Foot Ankle Int. 2013;34(3):365-371. PubMed | Google Scholar
- Dilip D Tanna, Prasoon Kumar, Mandeep S Dhillon. Nonunion of Medial Malleolus Fracture: Tension Band Wiring is an Effective Option Even in Failed Surgeries. Journal of Foot and Ankle Surgery (Asia Pacific). (2019). Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures




Article metrics

