
Bilateral choroidal metastasis revealing a breast carcinoma: a case report
Amine Mounsif, Oumayma El Mansouri, Houssaine Ait Lhaj, Mohamed Kriet, Fouad El Asri
Corresponding author: Amine Mounsif, Ophthalmology Department, Avicenne Military Hospital, Faculty of Medicine, Cadi Ayad University, Marrakesh, Morocco 
Received: 05 Jan 2024 - Accepted: 04 Feb 2024 - Published: 19 Feb 2024
Domain: Oncology, Ophthalmology, Surgical oncology
Keywords: Breast carcinoma, choroidal metastasis, multimodal imaging, case report
©Amine Mounsif et al. PAMJ Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Amine Mounsif et al. Bilateral choroidal metastasis revealing a breast carcinoma: a case report. PAMJ Clinical Medicine. 2024;14:21. [doi: 10.11604/pamj-cm.2024.14.21.42595]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com//content/article/14/21/full
Case report 

Bilateral choroidal metastasis revealing a breast carcinoma: a case report
Bilateral choroidal metastasis revealing a breast carcinoma: a case report
![]() Amine Mounsif1,&,
Amine Mounsif1,&, ![]() Oumayma El Mansouri1, Houssaine Ait Lhaj1, Mohamed Kriet1, Fouad El Asri1
Oumayma El Mansouri1, Houssaine Ait Lhaj1, Mohamed Kriet1, Fouad El Asri1
&Corresponding author
The incidence of ocular breast cancer metastatic disease varies from 5% to 30%, and these metastases occur in 77-90% of already-known cancer patients. The revealing forms and bilateral involvement remain exceptional. We report the case of a 42-year-old patient with a non-notable medical history who presented with a progressive decrease in visual acuity of the left eye. Fundus examination revealed a yellowish choroidal mass in the posterior pole with serous retinal detachment. Research on primitive objectified left breast carcinoma. The patient received chemotherapy before surgical intervention and ocular radiotherapy was administered in the left eye, with no significant response revealed on ultrasound control at 1 month after treatment. The staging of a breast tumor may require an ophthalmologic evaluation along with a fundus examination. Furthermore, when a choroidal secondary tumor is found, a thorough breast examination is necessary.

Studies have shown that the incidence of ocular breast cancer metastatic disease ranges from 5% to 30% And these metastases occur in 77-90% of previously diagnosed cancer patients [1,2]. The revealing forms and bilateral involvement remain exceptional [3]. The patient may exhibit floaters, flashes, reduced field of vision, and blurred vision [4,5]. A comprehensive systemic evaluation and high clinical suspicion are necessary for an accurate diagnosis of ocular metastases. On the basis of her ocular metastatic features, the patient in our case was diagnosed with systemic malignancy for the first time. We want to emphasize how crucial the ophthalmologist is in identifying a potentially fatal primary cancer. Early identification of cancer improves patients´ quality of life. We report a case characterized by bilateral and solitary (without other secondary locations) choroidal metastasis revealing breast neoplasia to emphasize the fact that the eye is a window to systemic diseases.

Patient information: a 42-year- old patient with a non-notable medical history presented to our hospital with a progressive decrease in visual acuity of the left eye lasting for more than 2 weeks that suddenly worsened in the last three days.
Clinical findings: on examination, the right eye had a best-corrected visual acuity (BCVA) of 20/20, whereas the left eye was at counting fingers. Anterior segment examination and intraocular pressure were normal in both eyes.
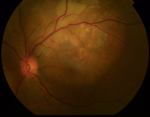
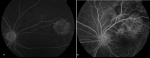
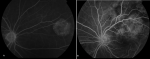
Diagnostic assessment: fundus examination revealed a normal optic nerve in the right eye and a small yellowish lesion in the nasal quadrant with a well-defined margin. The left eye fundus showed a yellowish choroidal mass in the posterior pole with a serous retinal detachment and overlying retinal pigment epithelium changes (Figure 1). B -scan oculo-orbital ultrasonography with a high-frequency probe showed an elevated mass lesion in the choroid on the right and left eye with moderate to high internal echogenicity measuring 2,87mm in the right eye (Figure 2 A, B). Fluorescein angiography in both eyes revealed an alternate hypofluorescent and hyperfluorescent pattern with multiple microaneurysms mimicking a typical “starry-sky” (Figure 3). Right eye optical coherence tomography (OCT) showed a subretinal hyporeflective space with a lumpy- bumpy appearance of the retinal pigment epithelium (RPE) and an elevated choroidal mass, whereas the left eye showed a subretinal hyporeflective space with an intraretinal cyst and a choroidal mass beneath the RPE (Figure 4 A-D). Clinical examination revealed a hard nodule in the left breast. Echo mammography revealed an irregular nodular opacity in the left supero-external quadrant measuring 2 cm. This opacity was rated ACR 4 (American College of Radiology). Nodule cytopuncture found an infiltrating ductal adenocarcinoma serum bilirubin (SBR) grade III, triple negative. There were no associated axillary lymphadenopathies, neither homo nor contralateral. Extension assessment for other metastases was negative (abdominal ultrasound, thoraco-abdominal CT scan, brain magnetic resonance imaging (MRI), and bone scintigraphy).
Diagnosis: after conducting all of these investigations, we were able to conclude that the fundus lesion was a metastasis from an invasive ductal breast adenocarcinoma classified TNM T2pN0cM1.
Therapeutic intervention: the patient received chemotherapy before surgical intervention, and four courses of ocular radiotherapy were administered in the left eye.
Follow-up and outcomes: no significant response was observed as the visual acuity was still counting finger and choroidal metastases persisted on the ultrasound control at 1 month after treatment.
Patient perspective: during treatment, the patient was satisfied with the level of care provided.
Informed consent: consent was obtained, and the patient was made aware that her medical records would be kept confidential.
Because of its abundant blood supply, the choroid is the most common location for ocular metastases from systemic carcinoma, followed by the orbit, iris, ciliary body, optic nerve, conjunctiva, and eyelid [4]. Breast cancer is the most commonly found primitive cancer, followed by lung cancer [6]. The incidence of choroidal metastases from breast cancer is reported to be 39-49% [7]. According to Shields and associates´ [8] analysis of 520 eyes with uveal metastases, the breast (47%), lung (21%), and gastrointestinal system (4%) were the primary tumor sites that most often occurred. Choroidal metastases revealing breast cancer remain very rare [4] because these secondary locations mainly complicate previously known mammary neoplasia [3,4]. In fact, in the vast series of Demirci et al. [4], which included 264 patients with uveal metastases associated with breast cancer, only seven patients (3%) were indicative of primary neoplasia.
Solitary forms (with no other systemic metastatic sites) are uncommon [3], whereas bilateral forms are exceptional [5]. However, note that in over half of the cases, contralateral eye involvement is still infra-clinical and would only be found by a systemic ocular examination [4]. Patients typically exhibit one or more of the following symptoms: floaters, flashes, ocular pain, altered field of vision, and blurred vision [4,6]. In 7% of cases, patients show no symptoms [4,9]. The visual acuity is usually ranging from 20/20 to 20/40 in 56%, from 20/40 to 20/200 in 29%, and from 20/400 to no light perception in 15% [4].
Magnetic resonance imaging is the most sensitive and specific examination for diagnosing orbital metastases. Nonetheless, in symptomatic individuals, it is typically discovered during a purposeful search using a contrasted tomography. The diagnosis of choroidal masses with vascular flow can be made with the aid of Doppler ultrasound. Breast lesions have high reflectivity and an irregular interior structure in ultrasonography due to the presence of solid epithelial nests or glandular structures, which function as echo-producing interfaces [10]. Management of these metastases is purely palliative to preserve satisfactory visual acuity, as the prognosis dramatically decreases after ocular metastasis. In the literature, the relative incidence of central nervous system metastasis was 6% in patients with breast cancer before the development of ocular metastasis, whereas it increased to 28% after the development of ocular metastasis [4]. This could represent either new metastasis or, more likely, metastasis that was present but subclinical at the time of ocular diagnosis.
This treatment is mostly based on external radiotherapy and systemic polychemotherapy adapted to the type of primary neoplasia [4,10]. In the literature, there are few reports about the response of uveal metastasis to systemic chemotherapy and radiotherapy. In 75%-85% of cases, radiotherapy yields a favorable response [4,10]. Surgery has no place in this treatment, and the limited attempts at tumor reduction in large metastases result in increased morbidity and mortality [5].
Even in the absence of ocular symptoms, an ophthalmological examination with a fundus eye is needed in the extension evaluation of breast cancer; similarly, breast inspection should be systematic in the presence of a single or double choroidal tumor.
The authors declare no competing interests.
Patient management: Amine Mounsif, Oumayma El Mansouri, Houssaine Ait Lhaj, Mohamed Kriet and Fouad El Asri. Data collection: Amine Mounsif and Oumayma El Mansouri. Manuscript drafting: Amine Mounsif. Manuscript revision: Houssaine Ait Lhaj, Mohamed Kriet, and Fouad El Asri. All authors approved the final version of the manuscript.
We thank all the clinical staff who participated in the treatment of the patient.
Figure 1: color fundus of the left eye: serous retinal detachment surrounding a choroidal mass with variably sized retinal pigment epithelium lesions
Figure 2: ocular ultrasound B-scan: choroidal mass lesion with moderate to high internal echogenicity, smaller in right eye (A) than left eye (B)
Figure 3: fluorescein angiography of both eyes: alternate hypofluorescent and hyperfluorescent pattern with multiple microaneurysms mimicking a typical “starry-sky”
Figure 4: optical coherence topography of both eyes; A, B) right eye showing a subretinal hyporeflective space with a lumpy-bumpy appearance of the retinal pigment epithelium and an elevated choroidal mass; C, D) left eye showing a subretinal hyporeflective space with an intraretinal cyst and a choroidal mass beneath the retinal pigment epithelium
- Nelson CC, Hertzberg BS, Klintworth GK. A histopathologic study of 716 unselected eyes in patients with cancer at the time of death. American Journal of Ophthalmology. 1983;95(6):788-793. PubMed | Google Scholar
- Biswas J, Ho TC, Bhavsar K. Bilateral metastasis to the retina, choroids and optic nerve from breast cancer: a clinicopathological case. Indian J Ophthalmol. 2007;55(1):71-2. PubMed | Google Scholar
- Wickremasinghe S, Dansingani KK, Tranos P, Liyanage S, Jones A, Davey C. Ocular presentations of breast cancer. Acta Ophthalmol Scand. 2007;85(2):133-42. PubMed | Google Scholar
- Demirci H, Shields CL, Chao AN, Shields JA. Uveal metastasis from breast cancer in 264patients. Am J Ophthalmol. 2003;136(2):264-71. PubMed | Google Scholar
- Zhang HR, Ma ZZ, Feng Y, Guo T. Clinical characteristics of choroidalmetastasis. Zhonghua Yan Ke Za Zhi. 2009 Apr;45(4):301-8. PubMed | Google Scholar
- Bloch RS, Gartner S. The incidence of ocular metastatic carcinoma. Arch Ophthalmol. 1971 Jun;85(6):673-5. PubMed | Google Scholar
- Ferry AP, Font RL. Carcinoma metastatic to the eye and orbit. I. A clinicopathologic study of 227 cases. Arch Ophthalmol 1974; 92:276-86. PubMed | Google Scholar
- Shields CL, Shields JA, Gross NE, Schwartz GP, Lally SE. Survey of 520 eyes with uveal metastases. Ophthalmology 1997;104:1265-1276. PubMed | Google Scholar
- Wiegel T, Kreusel KM, Bornfeld N, Bottke D, Stange M, Foerster MH et al. Frequency of asymptomatic choroidal metastasis in patients with disseminated breast cancer: results of a prospective screening programme. Br J Ophthalmol. 1998;82(10):1159- 61. PubMed | Google Scholar
- Grajales-Alvarez R, Gutierrez-Mata A. Orbital metastases from breast cancer: A retrospective analysis of 28 cases. Cancer Treat Res Commun. 2020;24:10018. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures

Article metrics

