
Prevalence and associated risk factors among women with oligohydramnios in third trimester: a cross-sectional survey at the Zonal Referral Hospital
Upendo Tulinagwe Kibona, Bariki Mchome, Raziya Gaffur, Joseph Mlay, Patricia Swai, Eusebius Maro, Lacatus Nyombi, Novacatus Chuma, Emanuel Chogo, Ibrahim Salum, Annanoela Urassa, Kenneth Bagandanshwa, John Lugata, Benjamin Shayo, Pendo Mlay
Corresponding author: Upendo Tulinagwe Kibona, Department of Obstetrics and Gynecology, Kilimanjaro Christian Medical University College, Moshi, Tanzania 
Received: 10 Dec 2024 - Accepted: 02 Feb 2025 - Published: 13 Feb 2025
Domain: Obstetrics and gynecology
Keywords: Oligohydramnios, risk factors, prevalence, third trimester
©Upendo Tulinagwe Kibona et al. PAMJ Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Upendo Tulinagwe Kibona et al. Prevalence and associated risk factors among women with oligohydramnios in third trimester: a cross-sectional survey at the Zonal Referral Hospital. PAMJ Clinical Medicine. 2025;17:17. [doi: 10.11604/pamj-cm.2025.17.17.46181]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com//content/article/17/17/full
Research 
Prevalence and associated risk factors among women with oligohydramnios in third trimester: a cross-sectional survey at the Zonal Referral Hospital
Prevalence and associated risk factors among women with oligohydramnios in third trimester: a cross-sectional survey at the Zonal Referral Hospital
![]() Upendo Tulinagwe Kibona1,&, Bariki Mchome1,2, Raziya Gaffur2, Joseph Mlay1,2, Patricia Swai1,2,
Upendo Tulinagwe Kibona1,&, Bariki Mchome1,2, Raziya Gaffur2, Joseph Mlay1,2, Patricia Swai1,2, ![]() Eusebius Maro1,2,
Eusebius Maro1,2, ![]() Lacatus Nyombi1, Novacatus Chuma1, Emanuel Chogo1,
Lacatus Nyombi1, Novacatus Chuma1, Emanuel Chogo1, ![]() Ibrahim Salum1, Annanoela Urassa1, Kenneth Bagandanshwa1,
Ibrahim Salum1, Annanoela Urassa1, Kenneth Bagandanshwa1, ![]() John Lugata1,
John Lugata1, ![]() Benjamin Shayo3,
Benjamin Shayo3, ![]() Pendo Mlay1,2
Pendo Mlay1,2
&Corresponding author
Introduction: oligohydramnios has been a topical issue in obstetrics and gynecology because of its associated grave perinatal outcomes and increased maternal operative interventions. Oligohydramnios is defined as the reduced amount of amniotic fluid volume relative to gestational age. The magnitude of this condition and its associated risk factors have not been well described in Tanzania, where ultrasound use to diagnose this condition is limited.
Methods: hospital-based analytical cross-sectional survey was conducted from September 2022 to February 2023, the study group was those with an amniotic fluid index of ≤ 5 cm, and the control group had an amniotic fluid index of 8-24.9 cm. Obstetric ultrasound performed by an expert radiologist. We excluded those with known rupture of membranes confirmed by sterile speculum examination and congenital malformations of the fetus. We used multivariable logistic regression analysis to identify factors associated with oligohydramnios. Data was entered in Excel and analyzed using Stata version 15.
Results: enrolled 381 participants, 70 (18.3%) had oligohydramnios. The mean age of the participants was 29 years with a standard deviation of 5.46, the majority of participants were multigravida (61.90%) with a gestational age of 37-40 weeks (72.43%) and had more than four antenatal visits (91.04%). Pre-eclampsia (aOR=5.77,95%CI:3.25-10.22;p=0.002) eclampsia (aOR=4.56,95% CI:1.11-18.76;p=0.035). Gestational diabetes (aOR=2.93, 95% CI: 1.17-7.35;p=0.02) were significantly associated with oligohydramnios.
Conclusion: oligohydramnios was detected in approximately 2 out of ten women who attended Kilimanjaro Christian Medical Center and was more reported in pregnancies with preeclampsia, eclampsia, and gestational diabetes. We recommend increased assessment for both high-risk and low-risk pregnancies for oligohydramnios by using ultrasound in order to help prompt detection and intervention.

Oligohydramnios has been a topical issue in obstetrics and gynecology because of its associated grave perinatal outcomes and increased maternal operative interventions [1]. Oligohydramnios is defined as the reduced amount of amniotic fluid volume relative to gestational age it presents a threat to the fetus due to the risk of umbilical cord compression, intra uterine growth restriction, low birth weight, fetal distress, and has been associated with increased rate of caesarean delivery to the mothers [2]. Previously clinicians used to rely on clinical evaluation to diagnose oligohydramnios by using abdominal palpation to determine fundal height but due to the advancement of technology assessment of fetus and amniotic fluid volume shifted from subjective impression to the present state in which relatively sophisticated judgement of fetal condition can be done based on reproducible measurement [3]. Sonographic diagnosis of oligohydramnios is usually based on AFI less than 5cm or a single deepest pocket of amniotic fluid below 2cm, using either technique a fluid pocket must be at least 1cm in width to be considered adequate [4].
Prevalence and risk factors of oligohydramnios vary worldwide with other countries having a high prevalence of 12% while others have a low prevalence of 1-5% and these depend on diagnostic criteria used together with the population under study whether its high risk or low-risk population [5]. The most common cause of oligohydramnios at term pregnancy is idiopathic, however placenta insufficiencies such as hypertensive disorders, intra uterine growth retardation, cardiac, renal, diabetic vasculopathy, abruption placenta, angiotensin-converting enzymes inhibitors medications and congenital malformation can contribute to its occurrence [6]. Ultrasound is not commonly used during routine ante-natal care in many low- and middle-income countries, the population rates of oligohydramnios and the associated outcomes in low-middle-income countries are largely unknown and this causes underreporting of oligohydramnios [7]. To date, the magnitude of this condition and its outcomes has not been described in Tanzania where ultrasound use to diagnose this condition in pregnancy is limited despite advances in technology. This study aimed to determine the prevalence and associated risk factors of oligohydramnios among women in the third trimester of pregnancy delivered at KCMC hospital.

Study design and setting: this research adopts a cross-sectional hospital based analytical approach. This study was conducted at Kilimanjaro Christian Medical Center (KCMC) in Moshi, Kilimanjaro from September 2022 to February 2023. Patients with oligohydramnios receive comprehensive care in multidisciplinary setting since is a referral center for northern Tanzania, KCMC serves more than 20 million people and boasts 650 beds and 100 wards, comprised of seven districts covering 13250 kilometer square, serving as a teaching hospital.
Study population: this study included both primigravida and multiparous. Participants were pregnant women in the third trimester of pregnancy admitted and delivered at the KCMC labor ward from September 2022 to February 2023. The study population comprised of singleton pregnant women with gestational age 28 weeks and above who remembered their last menstruation period correctly with 3 previous regular cycles or dating ultrasound at less than 20 weeks of gestational, with intact membranes and pregnant women with other medical conditions associated with oligohydramnios such as pre-eclampsia, gestational diabetes, eclampsia and chronic hypertension were included. We excluded pregnant women who had borderline amniotic fluid index 5.1cm-7.9cm and polyhydramnios (>25cm) and we also excluded those with oligohydramnios diagnosed prior to 28 weeks of gestational age. Sample size determination was calculated using a formula by Kish Leslie´s [8] to get the required minimum sample size. We used a proportion of patients with oligohydramnios from the study conducted in Uganda [9]. A proportion of 9.4% and standard deviation of 1.96 and maximum standard error set at 0.05, after calculation we obtained a minimum sample of participants to be 399 and we used convenience sampling method.
Data collection: we used structured questionnaires capturing social-demographic data, obstetric history, and associated medical conditions of the patient. Modified and adapted Swahili-translated versions of questionnaires were used. All women admitted to the labor ward on that particular day during the study period who met the criteria were asked for informed and written consent, and those who agreed underwent physical examination measuring of vitals blood pressure. Temperature, weight, height, random blood glucose, hemoglobin levels, urinalysis. Systemic examination was also performed per protocol. They were asked about social demographic data, obstetric history, and associated medical conditions in pregnancy, and they underwent obstetric ultrasound examination. To determine the amount of amniotic fluid index, questionnaires were filled through direct interviews conducted by the principal investigator; an obstetric ultrasound was performed at the labor ward by an expert radiologist with a certificate together with the principal investigator a trans abdominal ultrasound was performed. The patient was placed in a supine position, and standard fetal biometry was performed (BPP).
Using landmarks on the maternal abdomen, the uterus was divided into four quadrants right and left halves by linear nigral and upper and lower halves by an imaginary line across the midway between the fundus of the uterus and symphysis pubis. A linear transducer was placed on the abdomen along with the mother´s longitudinal axis and held perpendicular to the floor in the sagittal plane. The maximum vertical dimension of the largest fluid pocket in each quadrant was measured in millimeters. The measurement obtained from each quadrant was summed up to form an amniotic fluid index, the identified pocket was considered clear of umbilical cords and other small parts of the fetus placental localization, fetal lie and presence of growth restriction together with biophysical profile will be done. The study group was selected as those with AFI ≤5cm termed oligohydramnios and controls (normal) with AFI ≥8cm-24.9cm. Those with deranged parameters were induced or planned for caesarean section depending on gestation age and associated complications. Induction of labor was done after performing bishop score management was done according to patient presentation and following departmental management protocol and Tanzania standard treatment guidelines. Ultrasound machine specification qualified radiologist used Toshiba Ultrasound machine system AG/SA Switzerland, 12-inch monochrome display monitor, rating 12v +/- 3% =3.0A, serial no. (GM55603A00E), model no. (ISTYLE), PROBLE DETAILS- PVM-375AT, 3.75MHZ.
Definitions: independent variables were maternal and social demographic characteristics such as (age, marital status, residence, occupation, level of education, referral status) medical conditions (gestational diabetes, pre-eclampsia, eclampsia, chronic hypertension) obstetric history (gravidity, parity, ANC visits, AFI index). Dependent variables was amniotic fluid index less than 5cm (oligohydramnios).
Statistical analysis: data were entered, using Microsoft Excel software and transferred to statistical software (STATA Version 15.0) for data analysis. Data cleaning and error checking were done to enhance validity and consistency before data analysis. Descriptive statistics were presented in frequencies and percentages. Figure 1 was used to present the enrollment flow chart and Table 1 and Table 2 have been used to present the risk factors of oligohydramnios. Continuous variables have been presented in the mean. The risk factors that were found to be significant by the univariate logistic analysis were analyzed further by multivariate logistic regression analysis. Multivariate analysis was done for the most prevalent risk factors, which were pre-eclampsia, eclampsia and gestational diabetes to control for confounders. Odds ratio and 95% CI have been used to make an association. A p-value of less than 0.05 (two-tailed) was considered statistically significant.
Ethical consideration: informed and written consent was obtained from participants before enrolling in a study and also before doing obstetrics examination and ultrasound scan verbal consent was obtained. For women who were not able to read, the consent form was read to them by a resident. A unique serial number was used that identified the study participant instead of using names for confidentiality and privacy was observed throughout the examination. Women who were found with other conditions were treated as per Tanzania guidelines and KCMC protocols. An ethical clearance certificate N° 159/2022 was obtained from the Tumaini University College Research Ethical Committee before the initiation of the study and permission was obtained from Kilimanjaro Christian Medical Center and the Head of Department of Obstetrics and Gynecology Department. Privacy and confidentiality of the information obtained from the patients were observed.
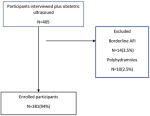
A total of 405 participants who met inclusion criteria were interviewed and underwent obstetrics ultrasound examination. Twenty four participants were excluded from the study. The remaining 381 participants were enrolled in the study, all of them agreed and signed their consent and this gives a participation rate of 100% as shown in Figure 1.
General characteristics of study participants: from 381 participants that were enrolled during the study period with a mean age of 29 years (SD=5.46+0.80) and age range between 16-41 years and the majority were married (74.28%) and aged 20-34 years old (76.11%) and among study participants. The majority were in secondary school education by (59%) most were residing in urban 287 (75.32%), and among those with oligohydramnios most of the participants were below age 20 years (25%) and among those without oligohydramnios majority were aged 20-34 (82.41%). The majority of participants with oligohydramnios were single (21.43%) and those with no oligohydramnios majority were married (82.69), out of those with oligohydramnios majority had primary level of education (28.00) and those with no oligohydramnios majority had college/university level of education (85.56%) (Table 1).
Obstetrics characteristics of the study participants: Table 2 showed that the majority of the participants were multigravida 2-3 by 236 out of 381 which is 61.94%. The majority of them were at term at the gestational age of 37-40 by 164 (43.04%) out of 381. Antenatal clinic attendance by participants was 91.07% and only 8.92% did not attend antenatal clinic, among those who attended ANC majority had more than 4 visits (55.64%), and the majority of the participants had a body mass index of less than 25kg by 92.1%. Among those with oligohydramnios majority were multigravida 2-3 (19.07%) while those with no oligohydramnios majority were grand gravida >4 (89.47%), most of the participants with oligohydramnios reported no antenatal clinic attendance 8 (23.53%) while those without oligohydramnios majority attended antenatal clinic 285 (82.13%).
Factors associated with oligohydramnios using univariable and multivariable logistic regression: the adjusted odds ratio in Table 3 below shows that pre-eclampsia (aOR=5.77, 95% CI: 3.25-10.22) eclampsia (aOR=4.56, 95% CI: 1.11-18.76). Gestational diabetes (aOR=2.93, 95% CI: 1.17-7.35), to be statistically associated with oligohydramnios after adjusting for confounders. Multigravida 2-3 (OR=1.05, 95% CI: 0.60-1.84), prime para (OR=1.09, 95% CI: 0.59-2.00), gestational age 33-36 (OR=1.01, 95% CI: 0.49-2.08) was found to be positively associated with oligohydramnios. However, this had no statistically significant.
This study aimed to determine the prevalence and associated risk factors of oligohydramnios among women in the third trimester delivered at KCMC hospital. Prevalence of oligohydramnios among women in the third trimester of pregnancy delivered at KCMC hospital was found to be 18.3% and risk factors which was found to be statistically significant were pre-eclampsia, eclampsia, and gestational diabetes. Our prevalence results were similar as findings from India (17%) [8]. This can be explained by the fact that both these studies were done in tertiary hospitals with a large sample size, and almost the same duration of follow-up was used. However, this prevalence is higher than what was reported in Uganda which was 9.4% [9] and this is because in our study we involved all pregnant women in the third trimester while in their study they involved only women of 36 weeks and above. A study from South Africa showed a prevalence of 23% [10] and their study considered only women who were referred due to post-term pregnancy. This explains the higher prevalence rate which was reported from this study and these differences in the prevalence can be explained by differences in the study population its high-risk or low-risk population, gestational age of study participants since all these have impacts on the prevalence so assessment of amniotic fluid index during pregnancy should be done to every pregnant woman during the third trimester of pregnancy using ultrasound to get the magnitude of oligohydramnios in hospitals and both complicated and uncomplicated pregnancies should be involved.
In our study, we found that risk factors associated with oligohydramnios were eclampsia at 7%, pre-eclampsia at 54%, gestational diabetes at 12%, post-term pregnancy was 3% and anemia in pregnancy at 24% and this was similar to the study conducted by Maryam A et al. found that pre-eclampsia is highly associated with oligohydramnios. Different results have been reported in India [11] which showed among women with oligohydramnios 24% had gestational diabetes, 16% had anemia, 12% had a pre-mature rupture, 12% had pre-eclampsia and 36% were non-maternal factors and this difference in the percentage of risk factors can be explained by different settings of the study and study population as we excluded women with pre-mature rupture in our study. Another study in Italy reported more than half of the participants had idiopathic causes of oligohydramnios [12]. This has been implicated when attending pregnant women in antenatal clinics, in both high-risk and low-risk pregnancies. This study has highlighted the magnitude and associated risk factors of oligohydramnios among women in the third trimester of pregnancy delivered at KCMC hospital. Our study generated valuable epidemiological data being one of the initial studies to estimate the magnitude of oligohydramnios in Tanzania and East African countries, but this study was prone to recall bias, especially when participants were supposed to provide information on their past medical and surgical history. We are unable to draw causal inferences from observed association due to the nature of the cross-sectional study. It was a single-center study in a zonal hospital, hence our findings cannot be generalizable in a general population but have helped to provide the bigger picture of the disease and showed the importance of ultrasound use in the diagnosis.
It has been found that the prevalence of oligohydramnios is 18.3% among women in the third trimester of pregnancy delivered at Kilimanjaro Christian Medical Center and the risk factors that are statistically significant associated with oligohydramnios are eclampsia, pre-eclampsia and gestational diabetes. Amniotic fluid assessments to determine oligohydramnios antepartum in the third trimester of pregnancy are important and will help to identify women who need increased antepartum surveillance for pregnancy complications of oligohydramnios. We recommend increased surveillance especially the use of ultrasound in the third trimester of pregnancy to detect oligohydramnios, especially among high-risk groups such as those with eclampsia, pre-eclampsia, and gestational diabetes to enable early detection of this condition to make timely intervention.
What is known about this topic
- Oligohydramnios has been associated with adverse perinatal and maternal outcomes;
- Early diagnosis and intervention have been associated with improved perinatal outcomes;
- Prevalence of oligohydramnios varies depending on the study population.
What this study adds
- This study has provided the magnitude of oligohydramnios among women delivered at KCMC hospital;
- It is the first published study in Tanzania and the second in East Africa;
- Outlined the risk factors associated with oligohydramnios in third trimester of pregnancy.
The authors declare no competing interests.
Conception and study design: Bariki Mchome and Pendo Mlay. Data collection: Ibrahim Salum, Kenneth Bagandanshwa. Data analysis and interpretation: Benjamin Shayo, Novacatus Chuma, Raziya Gaffur. Manuscript drafting: Upendo Tulinagwe Kibona, Annanoela Urassa, Lacatus Nyombi. Manuscript revision: Emanuel Chogo, John Lugata, Joseph Mlay, Eusebius Maro and Patricia Swai. Guarantor of the study: Upendo Tulinagwe Kibona. All the authors have read and agreed to the final manuscript.
We would like to give thanks and appreciate all specialists in the Department of Obstetrics and Gynecology for their teaching, support, constructive ideas, and directing me in the period of my studies. Special thanks to the head of the Department (my supervisor) Prof Pendo Mlay, for his time and input. Much appreciation to my beloved colleagues and fellow residents.
Table 1: social demographic characteristics of study participants with oligohydramnios (N=381)
Table 2: distribution of study participants obstetrics characteristics of oligohydramnios (N=381)
Table 3: multivariable logistic regression of the unadjusted odds ratio and adjusted odds ratio for the risk factors of oligohydramnios (N=381)
Figure 1: enrolment chart of study participants
- Teka H, Gidey H, Gebreezgabher T, Yemane A, Ebuy H, Berhe Y, Abate E. Determinants of maternal and neonatal outcomes of oligohydramnios after 37+ 0 weeks of gestation in mekelle public hospitals, northern Ethiopia. Mekelle: Research square. 2020 Aug 20. Google Scholar
- Jeyamani B, Anurekha JP, Arun Daniel J. Maternal and Perinatal outcomes of oligohydramnios in a tertiary care hospital in Salem, Tamil Nadu, India. Int J Reprod Contracept Obstet Gynecol. 2019 May 1;8:1939-42. Google Scholar
- Jagatia K, Singh N, Patel S. Maternal and fetal outcome in oligohydramnios- Study of 100 cases. Int J Med Sci Public Heal. 2013;2(3):724. PubMed | Google Scholar
- Bansal D, Deodhar P. A clinical study of maternal and perinatal outcome in oligohydramnios. J Res Med Den Sci. 2015 Oct 1;3(4):312-6.
- American College of Obstetricians and Gynecologists' Committee on Practice Bulletins-Obstetrics. ACOG Practice Bulletin No. 196: Thromboembolism in Pregnancy. Am Coll Obstet Gynecol. 2018;132(1Obstet Gynecol. 2018 Jul;132(1):e1-e17. PubMed | Google Scholar
- Dhakal RD, Paudel D. Factors associated with Oligohydramnios: age, hydration status, illnesses in pregnancy, nutritional status and fetal condition-a study from Nepal. Medical Science. 2017 Jul 30;5(2):26-31. Google Scholar
- Ogunlaja OA, Fawole AA, Adeniran AS, Adesina KT, Akande HJ, Ogunlaja IP et al. Ultrasound estimation of amniotic fluid and perinatal outcome in normotensive and pre-eclamptics at term in a Nigerian tertiary hospital. Journal of Medical and Biomedical Sciences. 2015;4(3):1-8. Google Scholar
- Rabie N, Magann E, Steelman S, Ounpraseuth S. Oligohydramnios in complicated and uncomplicated pregnancy: a systematic review and meta-analysis. Ultrasound Obstet Gynecol. 2017 Apr;49(4):442-449. PubMed | Google Scholar
- Figueroa L, McClure EM, Swanson J, Nathan R, Garces AL, Moore JL et al. Oligohydramnios: a prospective study of fetal, neonatal and maternal outcomes in low-middle income countries. Reprod Health. 2020 Jan 30;17(1):19. PubMed | Google Scholar
- Charan J, Biswas T. Review Article How to Calculate Sample Size for Different Study Designs in Medical Research. 2013;35(2). PubMed | Google Scholar
- Twesigomwe G, Migisha R, Agaba DC, Owaraganise A, Aheisibwe H, Tibaijuka L et al. Prevalence and associated factors of oligohydramnios in pregnancies beyond 36 weeks of gestation at a tertiary hospital in southwestern Uganda. BMC Pregnancy Childbirth. 2022 Aug 2;22(1):610. PubMed | Google Scholar
- Sathyapriya K, Sonal A, Venkateswaramurthy N, Sambathkumar R. Research on prevalence of oligohydramnios in third trimester of pregnancy and its outcome. International Journal of Life science and Pharma Research. 2019 Oct;9(4):7-13. Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures
Article metrics

