
Aural foreign bodies in children in a pediatric Senegalese hospital
Eric Joel Regonne, Abdou Sy, Malick Ndiaye, Yves Diandy, Mamadou Birame Faye, Bay Karim Diallo
Corresponding author: Eric Joel Regonneab, Otorhinolaryngology Department, Children´s Hospital of Diamniadio, Diamniadio, Senegal 
Received: 31 Oct 2019 - Accepted: 19 Jan 2020 - Published: 27 Jan 2020
Domain: Otolaryngology (ENT)
Keywords: Foreign bodies, ears, children, complications, otitis externa
©Eric Joel Regonne et al. PAMJ Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Eric Joel Regonne et al. Aural foreign bodies in children in a pediatric Senegalese hospital. PAMJ Clinical Medicine. 2020;2:25. [doi: 10.11604/pamj-cm.2020.2.25.20852]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com//content/article/2/25/full
Research 

Aural foreign bodies in children in a pediatric Senegalese hospital
Aural foreign bodies in children in a pediatric Senegalese hospital
Eric Joel Regonne1,2,&, Abdou Sy1, Malick Ndiaye1, Yves Diandy1, Mamadou Birame Faye3, Bay Karim Diallo4
1Otorhinolaryngology Department, Children's Hospital of Diamniadio, Diamniadio, Senegal, 2Otorhinolaryngology Department, Verdun Hospital Center, Verdun, France, 3Otorhinolaryngology Department, Principal Hospital, Dakar, Senegal, 4Otorhinolaryngology Department, Albert Royer Children's Hospital, Dakar, Senegal
&Corresponding author
Eric Joel Regonne, Otorhinolaryngology Department, Children's Hospital of Diamniadio, Diamniadio, Senegal
Introduction: aural foreign bodies (FB) are frequent in pediatric otorhinolaryngology and in pediatric emergencies. The objective of this study was to describe the socio-demographic, clinical and therapeutic aspects of aural FB in children in a pediatric hospital in Senegal.
Methods: this was a four-year hospital-based descriptive study performed in the Otorhinolaryngology Department of the Children's Hospital of Diamniadio, from 1st January 2013 to 31 December 2016 including all children under 15 years of age received for aural FB. The variables studied were age, gender, provenance, presenting symptom, time to consultation, the type of FB and morbidity.
Results: sixty three FB were extracted. Mean age was 6 years 4 months. Around fifty-two percent (52.4%) of patients were under 5 years old. There was a slight female predominance (32/63). Location was in the right ear canal in 55.6%. Seventy three percent of patients presented in our office were asymptomatic. The median time to consultation was 4 days. Within the first 24 hours after insertion, 22.2% of children presented to our office. Beads were the first FB (29.68%), followed by seeds and cotton (12.5% respectively). Foreign bodies' extraction were performed in consultation for 79.4% of patients. The morbidity was 20.6%. It was primarily otitis externa (8%). Myringoplasty was performed in one patient who had sequelae of tympanic membrane perforation.
Conclusion: aural FB is a common accident in under-5 year-olds. In our context there is a delayed consultation. Morbidity is similar to that of the literature.

Aural foreign bodies (FB) are a frequent complaint in otorhinolaryngology and pediatric emergencies [1]. They mainly concern children of less than 5 years [2-5]. According to the literature, 45 to 73% of children consult within the first 24 hours of insertion [3,6-8]. The types of FB depend on the socio-cultural context of the children. They are usually extracted in consultation. In some cases, extraction may be performed under general anesthesia when the child is not cooperating, when the FB is enclosed, or when the external auditory meatus has been traumatized during an unsuccessful extraction attempt. Complications are not exceptional; they occur in 0.7 to 47% of patients [4,7-10]. The objectives of this study were to describe the socio-demographic, clinical and therapeutic aspects of auricular foreign bodies in children presented in an otorhinolaryngology department of a pediatric hospital in Senegal.

We carried out a descriptive cross-sectional study including a 43-month retrospective phase from January 1, 2013 to July 31, 2016 and a 5-month prospective phase from August 1st to December 31st, 2016. It took place at the otorhinolaryngology department of the Children's Hospital of Diamniadio. It is a tertiary hospital located in a rural area, at 40 km from Dakar, the city capital of Senegal (West Africa). We included all patients aged less than 15 years who were diagnosed with unilateral or bilateral aural FB on clinical examination or complementary exams. Patients consulting with suspected aural FB that was not confirmed were not included. Extractions performed under general anesthesia were without intubation. The variables studied were: age, gender, provenance, presenting symptom, time to consultation, nature of FB, extraction method and complications. The data were recorded and analyzed using the SPSS (Statistical Package for Social Science) software, version 20. In the prospective phase, parental consent was obtained prior to inclusion. Data privacy was respected and patient names were not recorded in the data collection forms.
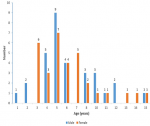
A total of 63 cases of auricular foreign bodies were included. Mean patient age was 6 years 4 months (SD, 3 years), median age was 5 years (range, 1 year to 15 years). Thirty-three patients (52.4%) were under 5 years of age. The modal age was 5 years (25.4%) (Figure 1). There was slight female predominance (32/63). There was no seasonal variation in the incidence of FB. Nine patients (14.3%) came from Diamniadio or its surroundings. In 35 patients (55.6%), the FB was located in the right ear, in 20 patients (31.7%) in the left and bilaterally in 8 children (12.7%). Table 1 shows the circumstances of aural FB discovery. In 46 cases (73.01%), the parents witnessed the insertion of the FB or children reported it to their parents or the FB were incidentally discovered during the consultation for another disease. Four children referred from a health center after an unsuccessful attempt to extract the FB presented with a laceration of the external auditory meatus. The consultation period was available for 40 patients (63.5%). It varied from one day to a 7 month, with a median time of 4 days. Fourteen children (22.2%) consulted within the first 24 hours of insertion. Table 2 shows the different FBs extracted. Aural FBs were mainly inorganic (73.4%). Beads were the first FBs (29.68%). A pure tone audiometry was performed in two patients before and after extraction. No deafness was found in these patients. Extraction was performed in 50 patients (79.4%) in our office and 13 (20.6%) in the theater under general anesthesia and spontaneous ventilation. Extraction under general anesthesia was indicated in 5 cases for enclosed FB, in 4 following failure of extraction in a health center, in 2 following failure of extraction in consultation, and for 2 patients because they were not cooperating. Thirteen patients (20.6%) had a complication after FB extraction. In five of them (8%) it was an otitis externa, which had evolved well with ear drops antibiotics. Four patients had tympanic membrane perforation. In three, it has completely closed; in the fourth, the perforation lasted more than 3 months. He underwent a myringoplasty. Three patients had a wound in the external auditory meatus that had evolved well. One patient had a hemotympanum that evolved favorably.
The insertion of a FB in the ear by a child is a common complaint in otorhinolaryngology and pediatric emergencies [1]. Most of children received in consultation for an aural FB are under 5 years of age [2-5, 10], with a mean age of 6 years 6 months [1, 9]. Our results corroborate those of the literature. According to the literature, there is a male predominance [1, 7, 9-11]. The girls were the most represented in our series. Predisposing factors for insertion of a FB into the ear identified by Ansley et al. [7] were: irritation of the external auditory meatus, otitis externa and acute otitis media, and to a lesser extent mental retardation and curiosity of children. Most FBs were found in the right ear. This result corroborates the literature [5, 9, 10, 12]. Afolabi et al. [5] in 2010 in Nigeria found a correlation between handedness of the patients and the location of the FB. In the literature, 45 to 73% of children consulted within the first 24 hours of insertion [3, 6-8]. In developing countries, there is a trend for delayed consultation. In Nigeria, 23 to 28% of children came within the first 24 hours [4, 5, 12]. Our study confirms this trend with 22.2% of children seen in consultation the first 24 hours. This delay in consultation in our context could be explained by: difficult access to the hospital, because the public transport services (bus or taxi) are deficient; people live far away from tertiary hospitals.
In our study, only 14.3% of patients were from Diamniadio. The others came from other towns or regions of Senegal, often more than 50 kilometers distance; the lack of financial resources: consultation fees are 3,000 FCFA (4.5 €), FB extraction in office 5,000 FCFA (7.62 €), FB extraction under general anesthesia 50,000 FCFA (76 €). For the inhabitants of this region, who are small traders or farmers, it is a significant financial cost, given that the gross domestic product per capita in Senegal in 2014 was 1,067$ US (42,651$ US in France and 54,306$ US in the United States the same year) [13]; neglect of parents. Shrestha et al. [14] in Kathmandu in 2012, showed that the delay in consultation was associated with parents´ low educational level. We did not evaluate this aspect in our work, but we believe it may be a cause of delayed consultation in our context. According to the literature, 10 to 95.8% of patients [4, 5, 9, 12, 15] are asymptomatic at admission either because parents witnessed the insertion of the FB or the child reports the accident to his parents. However, 2 to 90% of the children [4, 8, 9, 15, 16] consult for an otalgia, 1 to 30% for hearing loss [4, 8, 14, 15], 19.5% for an otorrhea [12], 4.3 to 21.2% for otorrhagia [12, 16] and 0.4% [15] for a feeling of blocked ear. There is a wide diversity of FBs, depending on the environment of the child and on the cultural habits of each country.
Fancy beads or small plastic beads and seeds are the main types of FBs in the literature [1, 4, 5, 15]. In our series, beads were the most commonly found FB. In our context, it is common to see children wear very soon necklaces or buckles usually made of beads or small plastic beads. They are also used as decorative accessories for women's clothing and prayer beads. Our result corroborates that of Dubois et al. [9] in France who found a predominance of beads (25%). We did not find any case of button battery. According to the literature, aural FBs are extracted in 70 to 96% in consultation, in a quiet and cooperating child using a hook or after washing the ear with a syringe [4, 7, 12]. In 4 to 30% of cases, extraction is performed under general anesthesia [4, 6, 7, 9, 17, 18]. It is indicated when the child is uncooperative, when the FB is enclosed in the external auditory meatus, after failure of several removal attempts resulting in an external auditory meatus trauma or in a case of blunt, hard and irregular FB [7, 9]. General anesthesia was used in 20.6% in our series. Complications occurred in 0.7 to 47% of patients [1, 4, 7-10, 17]. In our series, complications represented 20.6%. Wounds of the external auditory meatus are the most frequent complications in the literature. They occur in 10 to 31% of cases [4, 7, 9-11]. They may be due either to the introduction of the FB or its removal [9].
Three children (4.8%) in our series had a wound of the meatus following extraction and four (6.35%) presented in our office with a wound. Afolabi et al. [12] in Nigeria, found 19.5% of children with a laceration of the external auditory meatus at the consultation. This is a tricky situation in the medical care, because these children are traumatized during an unsuccessful attempt of removal. When they come to consultation, a new attempt of extraction may be difficult because of the painful memory of the previous one and the inflammation of the external auditory meatus, causing otalgia and enclosed more the FB. In our practice, in such cases, an ear drop antibiotic is prescribed with an oral analgesic. Then we see the child again after a week. If the FB is removable, extraction is done in consultation preferably using an otomicroscope, or failing that, by direct vision using a frontal light. Otherwise, the extraction is performed under general anesthesia. Otitis externa is found in 2 to 14% of cases according to the literature [4, 6, 7, 9, 17]. The patient has an otalgia with or without a purulent otorrhea [9]. It may be a complication of the FB extraction or reveal the FB. In our series, it revealed FBs in 15.9% of cases as an unilateral otalgia associated with a fetid and purulent otorrhea. It was the first complication after FBs extraction. Tympanic perforation is found in less than 6% of patients according to the literature [4, 7, 9, 16]. It may be related to the introduction of the FB in the ear canal or be the result of removal attempts by inexperienced practitioners [6, 11]. It was found in our series in 4 patients (6.35%). Ijaduola et al. [10] in Nigeria, who had one of the largest series of literature, found 52.5% of children with tympanic perforation with or without purulent otorrhea at the first consultation. In our socioeconomic context where there is a lack of ENT specialists and a difficult access to tertiary hospitals, initial medical care usually begins in the nearest health center. There, a removal attempt is performed by paramedical staff having little experience and poorly equipped. The small size of our population did not allow us to make strong comparisons between gender and between age groups, and to generalize our results.
Aural FBs are frequent in children specially those of less than 5 years. Our context of practice is marked by a delay in consultation related to the remoteness of specialized health structures, the lack of financial resources of populations and the neglect of parents. In addition, it is marked by a somewhat higher frequency of tympanic membrane perforations than in the literature. This work highlights the difficulties in access to health care of the populations in our region, their low socio-economic level and the lack of qualified personnel. It is therefore necessary to improve access to health care and socio-economic level of the population and to train health center staff who are the first to receive patients.
What is known about this topic
- Aural foreign bodies are frequent in children;
- Most of patients come to the emergencies in the first 24 hours of insertion.
What this study adds
- In our context there is a delayed consultation;
- The frequency of tympanic membrane perforation is higher than in the literature.
The authors declare no competing interests.
All authors participated in all stages of writing the manuscript (conception, acquisition of data, drafting of manuscript, correction). All the authors have read and agreed to the final manuscript.
Table 1: distribution of patients by discovery circumstances
Table 2: distribution of patients by foreign bodies' type
Figure 1: distribution of patients by age and gender
- DiMuzio J, Deschler DG. Emergency department management of foreign bodies of the external auditory canal in children. Otol Neurotol. 2002;23(4):473-475. PubMed | Google Scholar
- Mukherjee A, Haldar D, Dutta S, Dutta M, Saha J, Sinha R. Ear, nose and throat foreign bodies in children: a search for socio-demographic correlates. Int J Pediatr Otorhinolaryngol. 2011;75(4):510-512. PubMed | Google Scholar
- Hon SK, Izam TM, Koay CB, Razi A. A prospective evaluation of foreign bodies presenting in the ear, nose and throat clinic, hospital Kuala Lumpur. Med J Malaysia. 2001;56(4):463-470. PubMed | Google Scholar
- Ologe FE, Dunmade AD, Afolabi OA. Aural foreign bodies in children. Indian J Pediatr. 2007;74(8):755-758. PubMed | Google Scholar
- Afolabi OA, Salaudeen AG, Alabi BS, Lasisi AO. Correlation of aural foreign bodies with handedness: an observational study in a Nigerian tertiary hospital. J Clin Med Res. 2010;2:79-82. Google Scholar
- Balbani AP, Sanchez TG, Butugan O, Kii MA, Angélico FV Jr, Ikino CM et al. Ear and nose foreign body removal in children. Int J Pediatr Otorhinolaryngol. 1998;46(1-2):37-42. PubMed | Google Scholar
- Ansley JF, Cunningham MJ. Treatment of aural foreign bodies in children. Pediatrics. 1998;101(4 pt 1):638-641. PubMed | Google Scholar
- Baker MD. Foreign bodies of the ears and nose in childhood. Pediatr Emerg Care. 1987;3(2):67-70. PubMed | Google Scholar
- Dubois M, Francois M, Hamrioui R. Foreign bodies in the ear: Report of 40 cases. Arch Pediatr. 1998;5(9):970-973. PubMed | Google Scholar
- Ijaduola GTA, Okewo PA. Foreign body in the ear and its importance. J Trop Paediatr. 1986;32(1):4-6. PubMed | Google Scholar
- Bressler K, Shelton C. Ear foreign-body removal: a review of 98 consecutive cases. Laryngoscope. 1993;103(4 pt 1):367-370. PubMed | Google Scholar
- Afolabi O, Alabi B, Segun-Busari S, Dunmade A, Ologe F. Paediatric aural foreign bodies: a challenge to care givers. Internet J Otorhinolaryngol. 2008;11(1):1-5.
- United Nations Department of Economic and Social Affairs. Statistical Yearbook New York 59th issue. 2016.
- Shrestha I, Shrestha BL, Amatya RCM. Analysis of ear, nose and throat foreign bodies in Dhulikhel Hospital. Kathmandu Univ Med J. 2012;10(38):4-8. PubMed | Google Scholar
- Chai CK, Tang IP, Tan TY, Jong DEYH. A review of ear, nose and throat foreign bodies in Sarawak general hospital, a five year experience. Med J Malaysia. 2012:67(1):17-20. PubMed | Google Scholar
- Ngo A, Ng KC, Sim TP. Otorhinolaryngeal foreign bodies in children presenting to the emergency department. Singapore Med J. 2005:46(4):172-178. PubMed | Google Scholar
- Shafi M, Yousufani A, Hussain SI. Foreign bodies in external auditory canals: experience of 653 cases over 8 years. JLUMHS. 2010;9:70-75. Google Scholar
- Endican S, Garap JP, Dubey SP. Ear, nose and throat foreign bodies in Melanesian children: an analysis of 1037 cases. Int J Pediatr Otorhinolaryngol. 2006;70(9):1539-1545. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures
Article metrics

