
Collision of a basal cell carcinoma and a naevus
Samia Mrabat, Hanane Baybay, Sara Elloudi, Zakia Douhi, Fatima Zahra Mernissi, Abdelhafid El Marfi, Abdelmajid El Mrini, Mouna Rimani
Corresponding author: Samia Mrabat, Département of Dermatology, Université Hospital Hassan II, Fès, Morocco 
Received: 12 Oct 2019 - Accepted: 19 Jan 2020 - Published: 03 Feb 2020
Domain: Dermatology
Keywords: Basal cell carcinoma, dermoscopy, melanocytic naevus
©Samia Mrabat et al. PAMJ Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Samia Mrabat et al. Collision of a basal cell carcinoma and a naevus. PAMJ Clinical Medicine. 2020;2:30. [doi: 10.11604/pamj-cm.2020.2.30.20635]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com//content/article/2/30/full
Case report 

Collision of a basal cell carcinoma and a naevus
Collision of a basal cell carcinoma and a naevus
Samia Mrabat1,&, Hanane Baybay1, Sara Elloudi1, Zakia Douhi1, Fatima Zahra Mernissi1, Abdelhafid El Marfi2, Abdelmajid El Mrini2, Mouna Rimani3
1Department of Dermatology, Université Hospital Hassan II, Fes, Morocco, 2Department of Traumatology, Université Hospital Hassan II, Fes, Morocco, 3Hassan Center of Pathology, Rabat, Morocco
&Corresponding author
Samia Mrabat, Département of Dermatology, Université Hospital Hassan
II, Fes, Morocco
The association of contiguous or ‘collision´ tumours in the same biopsy sample is not rare and is often reported in the literature. The association of basal cell carcinoma (BCC) and naevus is very difficult to diagnose clinically. We report the case of a 63 years old man who presented with an asymmetric heterochromatic plaque of the shoulder. Pathology found a melanocytic naevus with a basal cell carcinoma.

Cutaneous neoplasms with two or more distinct cell populations are well documented entities that frequently represents a diagnostic challenge to both clinicians and pathologists. Multiple presentations regarding the co-existence of basal cell carcinoma with melanoma or melanocytic nevi have been reported [1]. Cutaneous collision tumours are extremely difficult to diagnose preoperatively, even with the help of dermoscopy, in particular when one of the lesions is melanocytic [2]. In the presence of nonmelanocytic collision lesions, such as seborrheic keratosis and BCC, the diagnosis is easier due to the presence of dermoscopic criteria that are evocative of either lesion [3].

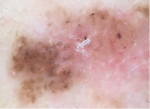
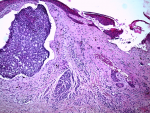
A 63-year-old patient with a history of chronic sun exposure and cutaneous bowen´s disease. Presented an asymptomatic skin lesion on his right shoulder that has been growing for the past three years. The dermatological examination showed an asymmetric heterochromatic plaque of 1.5 cm in diameter with irregular contours suggesting a suspicious pigmented lesion according to the ABCD rule (Figure 1). Dermoscopic analysis revealed the presence in the most pigmented portion of brown dots and globules crossed in the lower region by a hair. It also showed a regression area in the center, and ovoid nests with telangiectatic vessels in the less pigmented area (Figure 2). Giving the patient´s history and the suspicious nature of lesion both clinically and dermoscopically, we performed a surgical excision. The histological study showed tumor proliferation of basaloid-like cells at the periphery, with localized retraction slots, these cells sit within a dermal melanocytic tumor proliferation surrounded by a connective stroma harboring melanocytic pigment (Figure 3). The diagnosis of a collision tumour-basal cell carcinoma and dermal naevus was then established. No recurrence was found after two years of follow up.
Nomenclature of collision tumors is confusing. Satter et al simplified the terminology by classifying them as collision, combined, colonized, or biphenotypic tumors [4]. And so, the word collision tumor is defined as two distinct neoplasms that occur within close proximity of each other but maintain sharp distinct boundaries [4,5]. Combined tumors are neoplasms consisting of two phenotypically different, yet difficult to separate populations of malignant cells [4-6]. Biphenotypic tumors refer to very rare neoplasms that arise from a common stem cell precursor wich undergoes divergent differentiation. The tumor cell populations that arise exhibit overlapping immunohistochemical and molecular properties [7]. When melanoma in situ permeates an adjacent or underlying basocellular carcinoma tumor, it is called colonization. In these cases, atypical melanocytes from are found interspersed among basaloid epithelial cell aggregates [8]. Our patient ‘s histological examination found two adjacent cell populations but with clear and sharp boundaries hence the diagnosis of a collision tumour.
In our case, dermoscopy revealed two different patterns in the lesions: brown dots and globules crossed by a hair suggestive of a melanocytic naevus as well as ovoid nests with telangiectatic vessels wich are a common finding in pigmented basal cell carcinoma. Looking backward, we should have thought of the diagnosis of a collision tumour giving the presence of two distinct lesions.
The authors declare no competing interests.
All the authors have read and agreed to the final manuscript.
Figure 1: asymmetric heterochromatic plaque of the shoulder
Figure 2: dermoscopy showing pigmented globules and dots at the left and ovoid nests with telangiectatic vessels at the right
Figure 3: basal cell carcinomatous proliferation in the upper left + dermal nevocellular proliferation
- Mancebo SE, Marchetti MA, Hollmann TJ, Marghoob AA, Busam KJ, Halpern AC. Melanoma in situ colonizing basal cell carcinoma: a case report and review of the literature. Dermatol Pract Concept. 2015 Jan;5(1): 25-30. PubMed | Google Scholar
- de Giorgi V, Massi D, Sestini S, Alfaioli B, Carelli G, Carli P. Cutaneous collision tumour. Br J Dermatol. 2005 Apr;152(4):787-90. PubMed | Google Scholar
- Cosme Alvarez-Cuesta C, Vazquez-Lopez F, Perez-Oliva N. Dermatoscopy in the diagnosis of cutaneous collision tumour. Clin Exp Dermatol. 2004 Mar;29(2):199-200. PubMed | Google Scholar
- Satter EK, Metcalf J, Lountzis N, Elston DM. Tumors composed of malignant epithelial and melanocytic populations: a case series and review of the literature. J Cutan Pathol. 2009;36(2):211-19. PubMed | Google Scholar
- Cornejo KM, Deng AC. Malignant melanoma within squamous cell carcinoma and basal cell carcinoma: is it a combined or collision tumor? a case report and review of the literature. Am J Dermatopathol. 2013 Apr; 35(2):226-34. PubMed | Google Scholar
- Miteva M, Herschthal D, Ricotti C, Kerl H, Romanelli P. A rare case of a cutaneous squamomelanocytic tumor: revisiting the histogenesis of combined neoplasms. Am J Dermatopathol. 2009 Aug;31(6):599-603. PubMed | Google Scholar
- Rosen LB, Williams WD, Benson J, Rywlin AM. A malignant neoplasm with features of both squamous cell carcinoma and malignant melanoma. Am J Dermatopathol. 1984 Summer;6 Suppl:213-9.. PubMed | Google Scholar
- Wang H, Benda PM, Piepkorn MW. Parasitism of basal cell carcinoma by lentigo maligna melanoma. J Am Acad Dermatol. 2003 May; 48(5 Suppl):S92-4. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures

Article metrics
PlumX Metrics
Collision of a basal cell carcinoma and a naevus
