
Crossed fused renal ectopia: a rare congenital malformation
Soufiane Ennaciri, Khalid Ouatar, Mustapha Ahsaini, Soufiane Mellas, Jalal Eddine El Ammari, Med Fadl Tazi, Med Jamal El Fassi, My Hassan Farih
Corresponding author: Soufiane Ennaciri, Urology Department, Hassan II University Hospital, Fes, Morocco 
Received: 17 Feb 2020 - Accepted: 26 Feb 2020 - Published: 27 Feb 2020
Domain: Urology
Keywords: Crossed ectopia, renal fusion, fortuitous discovery
©Soufiane Ennaciri et al. PAMJ Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Soufiane Ennaciri et al. Crossed fused renal ectopia: a rare congenital malformation. PAMJ Clinical Medicine. 2020;2:73. [doi: 10.11604/pamj-cm.2020.2.73.21846]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com//content/article/2/73/full
Case report 

Crossed fused renal ectopia: a rare congenital malformation
Crossed fused renal ectopia: a rare congenital malformation
Soufiane Ennaciri1,&, Khalid Ouatar1, Mustapha Ahsaini1, Soufiane Mellas1, Jalal Eddine El Ammari1, Med Fadl Tazi1, Med Jamal El Fassi1, My Hassan Farih1
1Urology Department, Hassan II University Hospital, Fes, Morocco
&Corresponding author
Urology Department, Hassan II University Hospital, Fes, Morocco
Crossed fused renal ectopia is a rare congenital malformation, in which the two kidneys are on the same side with one of the ureters and fusion between the two parenchyma. The ureter of the ectopic kidney crosses the midline and implants normally in the bladder. This anomaly is most often asymptomatic and of incidental discovery. We report the case of a patient without similar cases in his family, presenting a crossed fused renal ectopia discovered fortuitously during a prostate hypertrophy assessment.

Crossed fused renal ectopia (CFRE) is defined by the presence of one of the two kidneys on the contralateral side with a fusion between the two parenchyma. The ureter of the ectopic kidney crosses the midline and implants normally in the bladder. We report an observation of a patient in which we accidentally discovered an CFRE.

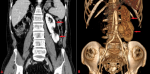
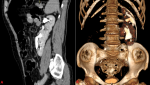
It´s about a 62-year-old patient, with no previous medical history, who presented to consultation for lower urinary tract symptoms evolving in recent months, such as dysuria, day and night pollakiuria at the rate of four night-awakening. The clinical examination did not find any sensitivity or lumbar contact. The digital rectal found an about 50g normally rubbery and smooth prostate. On the laboratory tests, the serum creatinine was 12 mg/l and the urine cytobacteriological exam was normal. A renovesico-prostatic ultrasound was performed, showing no visualization of the right kidney and a left kidney increased in volume with a duplication of the excretory system and without dilation of the pyelocaliciel cavities. The bladder was thin-walled and the prostate was homogeneous, but enlarged, measuring 58 ml. The post-void residual was 66 ml. The imaging was supplemented by a CT scan which revealed a crossed renal ectopia and fusion of the parenchyma of the two kidneys (Figure 1), the upper kidney being disrotated and the ureter of the lower kidney crossing the midline, just below the aortic bifurcation to get normally into the bladder on the right side (Figure 2). Our approach was to start an alpha blocker therapy for his benign prostatic hyperplasia, with ultrasound monitoring of the CFRE as there were no complications.
Crossed fused renal ectopia is a rare birth defect. It is due to an abnormality in the embryonic development of the ureteral bud and metanephric blastema, between the fourth and the eighth week of gestation [1]. Its frequency is around 1/7000 with a male predominance (3/2) [2,3]. It is characterized by the presence of two kidneys on the same side. In 90% of these cases, the crossed ectopic kidney is fused to the orthotopically located kidney. Indeed, this fusion is often made between the upper pole of the kidney in ectopia and lower pole of the normally positioned kidney, we then talk about lower cross renal ectopia [3], which is the case for our patient. The ureter crosses the midline and joins the corresponding meatus. CFRE may remain asymptomatic until it is accidentally discovered on a radiological examination for another reason. In the case of our patient, the diagnosis was made during a prostate hypertrophy assessment. However, CFRE can be manifested by unclear abdominal pain, pyuria. Hydronephrosis and the occurrence of calculus can explain these symptoms and would be favored by a drainage failure (lack of kidney position, vascularization abnormality crossing the excretory system). In one third of the cases, the diagnosis is made in front of an asymptomatic abdominal mass [4]. Ultrasound is the initial examination that guides the diagnosis and looks for possible complications such as lithiasis and dilation of the excretory tract. The CT urography confirms the diagnosis and allows a better anatomical study, especially for the individualization of the tow ureters delivery [5]. The evolution of this abnormality is favorable without alteration of renal function or blood pressure [6]. However, the risk of complications, especially lithiasis, is not negligible [7].
The CFRE is generally asymptomatic and of incidental discovery. Ultrasonography is the first line examination. The uroscanner offers a better anatomical study. Therapeutic management is based on abstention in the absence of complications.
The authors declare no competing interests.
All the authors have read and agreed to the final manuscript.
Figure 1: angioscan images, coronal section (A) and 3D reconstruction (B) showing the fusion of the two renal parenchyma
Figure 2: CT images in excretory time, sagittal section (A) and 3D reconstruction (B) showing fused cross renal ectopia. The normal kidney being disrotated and the ureter of the ectopic kidney crossing the midline above the promontory
- Elumalai G, Sakyi EA. Congenital anomalies of the kidney embryological basis and its clinical importance. 2017;5. Google Scholar
- Bhatnagar V, Gupta A, Kumar R, Solanki S. Crossed fused renal ectopia: challenges in diagnosis and management. J Indian Assoc Pediatr Surg. 2013;18(1):7-10. PubMed | Google Scholar
- Kalfa N, Veyrac C, Dubois C, Morin D, Lopez C, Averous M. Malformations congénitales du rein. EMC - Urol. 2009;2(3):1-20.
- Gleason PE, Kelalis PP, Husmann DA, Kramer SA. Hydronephrosis in renal ectopia: incidence, etiology and significance. J Urol. 1994;151(6):1660-1661. PubMed | Google Scholar
- Glodny B, Petersen J, Hofmann KJ, Schenk C, Herwig R, Trieb T et al. Kidney fusion anomalies revisited: clinical and radiological analysis of 209 cases of crossed fused ectopia and horseshoe kidney. BJU Int. 2009;103(2):224-235. PubMed | Google Scholar
- van den Bosch Caroline MA, van Wijk Joanna AE, Beckers Goedele MA, van der Horst Henricus JR, Schreuder Michiel F, Bokenkamp Arend. Urological and Nephrological Findings of Renal Ectopia. J Urol. 2010;183(4):1574-1578. PubMed | Google Scholar
- Boatman DL, Culp Jr DA, Flocks RH. Crossed renal ectopia. J Urol. 1972;108(1):30-1. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures
Article metrics

