
Acute cholecystitis that must not be operated
Atef Mejri, Khaoula Arfaoui
Corresponding author: Atef Mejri, General Surgery Department, Jendouba Regional Hospital, Jendouba, Tunisia 
Received: 20 Feb 2020 - Accepted: 26 Feb 2020 - Published: 02 Mar 2020
Domain: Infectious disease,General surgery
Keywords: Cholecystitis, viral hepatitis, surgery
©Atef Mejri et al. PAMJ Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Atef Mejri et al. Acute cholecystitis that must not be operated. PAMJ Clinical Medicine. 2020;2:80. [doi: 10.11604/pamj-cm.2020.2.80.21910]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com//content/article/2/80/full
Case report 

Acute cholecystitis that must not be operated
Acute cholecystitis that must not be operated
Atef Mejri1,&, Khaoula Arfaoui1
1General Surgery Department, Jendouba Regional Hospital, Jendouba, Tunisia
&Corresponding author
Atef Mejri, General Surgery Department, Jendouba Regional Hospital, Jendouba, Tunisia
Viral hepatitis A still endemic in African continent and this type of hepatitis can be complicated by an acute cholecystitis that is a common pathology in surgery. Acute cholecystitis imposes usually urgent management including a cholecystectomy, the only guarantee that can save the vital prognosis. However, a particular form of acute cholecystitis seems to particularly affect the African continent and is an exception to this rule. This work illustrates the case of a form of acute cholecystitis for which it was necessary to avoid any surgical procedure and that had a good outcome after a successful conservative management.

It is commonly admitted that acute cholecystitis is a diagnostic and therapeutic emergency. However, there is not an "acute cholecystitis" but there are "acute cholecystitis". In fact, the two main chapters of acute cholecystitis are: acute lithiasic cholecystitis whose positive diagnosis, etiology and management are well codified by professional recommendations (the Tokyo guidelines 2013); acute non-lithiasic cholecystitis (ANC) which, in addition to the problems of diagnosis (particularly etiological) pose problems in matters of management and for some forms of them cholecystectomy is prohibited. We expose through this presentation a form of acute cholecystitis in which cholecystectomy should be avoided because it only worsens the patient's situation.

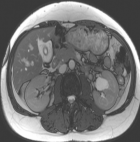
Mrs AE, 56 years old, consulted in emergency room for epigastric and right hypochondrium pain continuously evolving for 4 days. No scratch, blood transfusion or recent drug intake history were reported. Otherwise, the patient was not cholecystectomised. A clinical examination found jaundice, a body temperature at 37.8oC with a guarding at the right hypochondrium. Blood tests showed WBC: 3.9 x 109/ l, CRP: 7.7 mg/l and high bilirubin level, total bilirubin: 182.3 umol/l, conjugated Bilirubin: 165.5 umol/l. An abdominal ultrasound imaging was realized which describes an acute non-lithiasic cholecystitis (Figure 1) with perivesicular effusion and discreet dilation of the intrahepatic bile ducts. The patient underwent MRI scan showing that the gallbladder was non-lithiasic with a thickening of the vesicular walls (Figure 2), infiltration of the liver bed and around the intra and extra hepatic bile ducts. Neither bile ducts, nor Wirsung dilatation were detected. There was also no lesion in the pancreas. The rest of the biological tests found significant cytolysis, AST: 3817 IU/l; ALT: 4185 IU/l. Through this clinical case and despite the age of the patient, the diagnosis of acute non-lithiasic cholecystitis due to viral hepatitis A was strongly suspected. We performed the serology of hepatitis and our diagnosis was confirmed by a high level of HAV IgM antibody. An expectant attitude was then adopted with clinical and biological monitoring. The patient's condition was gradually improving with disappearance of the pains and progressive normalization of the biological tests.
Viral hepatitis A is an immunizing disease that is linked to lack of potable water and inadequate sanitation and hygiene (mainly dirty hands). This explains why it frequently touches children and it is an epidemic in Africa. It is rarely reported among adults but it is not exceptional. Extra hepatic complications of hepatitis A are nephrological (acute renal failure, glomerulonephritis) [1], but they can also touch the gallbladder. Viral infections (VHA and EBV) are responsible for the majority of acute children´non lithiasic cholecystitis [2] and must be mentioned in every case of ANC regardless of age, especially if traveling to endemic countries is reported and in the absence of vaccination. Mourani et al. reported the presence on immuno-histochemical examination, of VHA antigen in the gallbladder wall in a patient presenting ANC during VHA [3]. This confirms a direct link between VHA and ANC. Moreover, Juttner et al. showed that the degree of cytolysis appears to influence the degree of thickening of gallbladder wall [4]. The presence of major cytolysis in case of acute non-lithiasic cholecystitis, especially in Africa must always be a reminder of viral hepatitis A as an etiology and encourage performing VHA serology to confirm the diagnosis. In this case, the cholecystectomy should be avoided [5] because of the possible complications of this surgical procedure such as biliary ducts or vascular traumatic injuries and non-specific complications such as surgical wound infections and bedsore complications. Besides anesthetic drugs can be responsible as well of liver toxicity [6]. All of these increase liver damage and can be life threatening. In case of a non-contributive ultrasound imaging or clinical warning signs, CT scan must be performed in order to avoid wrong diagnosis and detect a gangrenous form imposing a change in therapeutic measures [7].
To sum up, in the presence of an acute non-lithiasic cholecystitis, the viral etiology is suspected in the presence of significant cytolysis and is sustained by serology results. In such an eventuality, cholecystectomy can be a source of complications for a patient whose liver is already suffering. Monitoring and symptomatic treatment usually improves the patient condition and contribute to a clinical, biological and radiological normalization.
The authors declare no competing interests.
All the authors have read and agreed to the final manuscript.
Figure 1: ultrasound imaging showing a non-lithiasic gallbladder with thickened walls
Figure 2: a MRI axial view of the abdomen showing a significant thickening of the gallbladder wall
- Paul Casha, Hervé Rifflet, Christophe Renou. Cholécystite aiguë alithiasique et hépatite virale A. Gastroentreol Clin Biol. 2000.
- Poddighe D, Sazonov V. Acute acalculous cholecystitis in children. World J Gastroenterol. 2018;24(43):4870-9. PubMed | Google Scholar
- Gora-Gebka M, Liberek A, Bako W, Szarszewski A, Kaminska B, Korzon M. Acute acalculous cholecystitis of viral etiology-a rare condition in children. J Pediatr Surg. 2008;43(1):e25-7. PubMed | Google Scholar
- Juttner HU, Ralls PW, Quinn MF, Jenney JM. Thickening of the gallbladder wall in acute hepatitis: ultrasound demonstration. Radiology. 1982;142(2):465-6. PubMed | Google Scholar
- Souza LJ de, Braga LC, Rocha N de SM. Acute acalculous cholecystitis in a teenager with hepatitis a virus infection: a case report. Braz J Infect Dis. 2009;13(1):74-6. PubMed | Google Scholar
- Herrine SK. Dysfonctionnement h�patique post-op�ratoire - Troubles h�patiques et biliaires. 2018. Le Manuel MSD. Accessed on 16 October 2019.
- Black MM, Mann NP. Gangrenous cholecystitis due to hepatitis A infection. J Trop Med Hyg. 1992;95(1):73-4. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures

Article metrics
PlumX Metrics
Acute cholecystitis that must not be operated
