
Ingestion of hydrochloric acid in adults
Hanane Delsa, Anass Nadi
Corresponding author: Hanane Delsa, Gastroenterology Unit, Cheikh Khalifa International Hospital, Faculty of Medicine Mohammed VI University of Health Sciences (UM6SS), Casablanca, Morocco 
Received: 23 Jun 2020 - Accepted: 03 Jul 2020 - Published: 09 Jul 2020
Domain: Gastroenterology,Intensive care medicine
Keywords: Caustic ingestion, esophagogastroduodenoscopy, hydrochloric acid, gastritis, Di-Costanzo classification
©Hanane Delsa et al. PAMJ Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Hanane Delsa et al. Ingestion of hydrochloric acid in adults. PAMJ Clinical Medicine. 2020;3:100. [doi: 10.11604/pamj-cm.2020.3.100.24527]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com//content/article/3/100/full
Images in clinical medicine 

Ingestion of hydrochloric acid in adults
Ingestion of hydrochloric acid in adults
Hanane Delsa1,&, Anass Nadi1
&Corresponding author

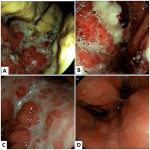
Corrosive ingestion is more common in the pediatric population (mostly accidents), but adults are also concerned (suicide) with more severe lesions. Massive ingestion of corrosive agents results in severe upper gastrointestinal and oropharyngeal tract injuries requiring multidisciplinary management. The endoscopy is systematic, the gastro-intestinal endoscopy must be conducted under sedation, with minimal insufflation, between 6 to 24 hours after ingestion. Endoscopic injuries must be described according to the Zargar or the Di-Costanzo classification. We report a case describing an ingestion of a strong acid. A 52-year-old woman, with no medical history especially psychiatric illness, was admitted to the emergency room for the voluntary ingestion of half a glass of hydrochloric acid for autolytic purposes after family problems. The patient was admitted to intensive care, she presented with a cough, hypersiallorhea, with epigastralgia, a thoracoabdominal computed tomography (CT) was conducted and objected a circumferential parietal thickening of the gastric wall in relation with post caustic ulcerative oedematous lesions. Twelve hours later, the esophagogastroduodenoscopy was performed and found a stage I esophagitis, a stage IIIA gastritis according to Di Costanzo (A,B). The medical treatment instaured: digestive rest, proton pump inhibitor and parenteral nutrition. The first endoscopic check was made after a week and showed an improvement in the endoscopic lesions: normal esophagus, fundic gastritis stage IIB and antral gastritis stage IIA according to the classification of Di-Costanzo. Psychiatric follow-up has been instituted. The evolution was favourable, the third endoscopic control after 2 weeks showed the healing of the lesions: antral gastritis stage IIA (C), Fundic gastritis stage I (D) of Di-Costanzo.
Figure 1: endoscopic image of caustic gastritis according to Di Costanzo: antral gastritis stage IIIA (A), fundic gastritis stage IIIA (B), antral gastritis stage IIA (C) and fundic gastritis stage I (D)
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Article metrics
PlumX Metrics
Ingestion of hydrochloric acid in adults
