
Mediastinal plasmocytoma with multiple myeloma: unusual presentation
Nouama Bouanani, Sophia Berrada
Corresponding author: Nouama Bouanani, Hematology and Stem Cell Transplant Department, Blood Transfusion and Cellular Therapy, Cheikh Khalifa International University Hospital, Casablanca, Morocco 
Received: 10 Jun 2020 - Accepted: 24 Jul 2020 - Published: 05 Aug 2020
Domain: Oncology
Keywords: Multiple myeloma, plasmocytoma, extramedullary
©Nouama Bouanani et al. PAMJ Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Nouama Bouanani et al. Mediastinal plasmocytoma with multiple myeloma: unusual presentation. PAMJ Clinical Medicine. 2020;3:162. [doi: 10.11604/pamj-cm.2020.3.162.24211]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com//content/article/3/162/full
Images in clinical medicine 

Mediastinal plasmocytoma with multiple myeloma: unusual presentation
Mediastinal plasmocytoma with multiple myeloma: unusual presentation
Nouama Bouanani1,2,&, Sophia Berrada3
&Corresponding author

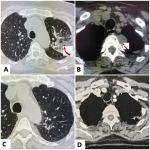
We report a rare case about a 60 years old Moroccan woman with a past medical history of gastrointestinal tuberculosis, admitted to the emergency department with fever, coughing, weight loss, spontaneous sternum fracture, back and chest pain. A physical examination revealed diffuse bone pain on palpation. Laboratory testing revealed anemia at 9 g/dl, high serum viscosity (80 mm/h). C-reactive protein at 100 mg/l. Serum protein electrophoresis showed monoclonal spike (30g/dL) in the gamma zone. Serum immunofixation study revealed a IgG lambda monoclonal paraprotein. Serum free light chains (kappa/lambda ratio: 0.04). Total protein level (88g/L). Twenty-four hours proteinuria was negative, complete metabolic panel, blood calcium and serum creatinine were normal. Bone marrow aspiration was performed and showed mature and dystrophic plasma cells at 38%. Computerised tomography scan of the chest revealed left broncho-pulmonary focus associated to a sternal fracture (A), mediastinal tissue mass of superior and posterior mediastinum of 30mm diameter (B), scanner-guided biopsy confirmed plasmocytoma, bronchoscopy with biopsy which objectified an inflammatory lesion. Hematological assessment concluded to mediastinal plasmocytoma with multiple myeloma Ig G Lambda. The Revised International Staging System is at 2. The patient received empirical antimicrobial therapy with good response, then she was treated with VTD protocol (bortezomib, thalidomide and dexamethasone), achieving complete remission followed by autologous stem cell transplantation (C,D). Consolidation therapy and maintenance are planned to maintain remission.
Figure 1: A) computerised tomography of the chest: lung window showing left broncho-pulmonary focus; B) computerised tomography of the chest with axial section showing mediastinal tissue mass of superior and posterior mediastinum, of 30mm diameter, adjacent to T2, well limited, homogeneous, without bone lysis, calcifications or necrosis; C) CT chest after treatement: disappearance of lung bronchopulmonary focus; D) computerised tomography of the chest after treatement: disappearance tissue mass of mediastinium
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Article metrics

