
Empyema thoracis in a patient with Enterococcus faecium bacteremia
Chee Yik Chang
Corresponding author: Chee Yik Chang, Medical Department, Hospital Sultanah Aminah, Jalan Persiaran Abu Bakar Sultan, 80100 Johor Bahru, Johor, Malaysia 
Received: 16 May 2020 - Accepted: 27 May 2020 - Published: 28 May 2020
Domain: Infectious disease
Keywords: Enterococcus faecium, empyema, vancomycin
©Chee Yik Chang et al. PAMJ Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Chee Yik Chang et al. Empyema thoracis in a patient with Enterococcus faecium bacteremia. PAMJ Clinical Medicine. 2020;3:30. [doi: 10.11604/pamj-cm.2020.3.30.23568]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com//content/article/3/30/full
Images in clinical medicine 

Empyema thoracis in a patient with Enterococcus faecium bacteremia
Empyema thoracis in a patient with Enterococcus faecium bacteremia
Chee Yik Chang1,&
1Medical Department, Hospital Sultanah Aminah, Jalan Persiaran Abu Bakar Sultan, 80100 Johor Bahru, Johor, Malaysia
&Corresponding author
Chee Yik Chang, Medical Department, Hospital Sultanah Aminah, Jalan Persiaran Abu Bakar Sultan, 80100 Johor Bahru, Johor, Malaysia

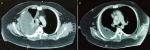
A 30-year-old male with a background of diabetes mellitus, hypertension, and obesity presented with a 2-week history of cough, associated with fever and breathlessness for one day. Auscultation of the lung revealed markedly reduced breath sound of the right lung. Contrast-enhanced CT of the thorax showed a gross right pleural effusion with associated atelectasis of the entire right lung (A). A pleural pigtail catheter was inserted in which a copious amount of purulent material was drained. Transthoracic echocardiography revealed normal cardiac contractility with the absence of vegetation. His blood culture yielded Enterococcus faecium, only susceptible to vancomycin, while cultures of the pleural fluid and sputum were negative. As a result, he was treated with intravenous vancomycin, with dosage adjustment made based on the therapeutic drug monitoring (aim for trough level = 15-20mg/L). His condition improved with intravenous vancomycin, which was given for a total duration of 6 weeks. Repeated thoracic CT at a one-month interval showed improving right pleural effusion (B). He was also referred to the cardiothoracic surgeon for decortication because of the residual empyema. E. faecium is a Gram-positive, commensal bacterium inhabiting the gastrointestinal tracts of humans and other mammals. E. faecium is a rare cause of empyema. This case illustrates the development of E. faecium empyema in a young patient with multiple co-morbid conditions. Pleural space infection caused by E. faecium requires pleural drainage and intravenous vancomycin for treatment.
Figure 1: (A) CT of the thorax shows a gross right pleural effusion; (B) CT of the thorax shows residual right pleural effusion, predominantly at the posterior aspect
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures
Article metrics

