
Catastrophic optic canal fracture
Hassan Baallal, Ali Akhaddar
Corresponding author: Hassan Baallal, Department of Neurosurgery, Avicenne Military Teaching Hospital, University Caddi Ayyad, Marrakech, Morocco 
Received: 20 May 2020 - Accepted: 27 Jun 2020 - Published: 29 Jun 2020
Domain: Maxillofacial surgery,Neurosurgery
Keywords: Fracture, optic canal, optic nerve
©Hassan Baallal et al. PAMJ Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Hassan Baallal et al. Catastrophic optic canal fracture. PAMJ Clinical Medicine. 2020;3:76. [doi: 10.11604/pamj-cm.2020.3.76.23647]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com//content/article/3/76/full
Images in clinical medicine 

Catastrophic optic canal fracture
Catastrophic optic canal fracture
Hassan Baallal1,&, Ali Akhaddar 1
&Corresponding author

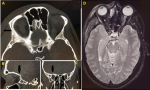
Isolated orbital roof fractures are raremost of these fractures heal without any complications. Traumatic optic neuropathy (TON) is one of the rare but catastrophic complications of orbital roof fractures. A 37-year-old gentleman was admitted in our emergency department following road traffic accident. He fell down from a motorcycle, on presentation to the emergency department he felt a little drowsy, had vomited twice, and complained of pain around his right eye. His Glasgow Coma Scale was 15/15. Clinical examination revealed right periorbital hematoma with edematous lids closing the right eye and ecchymosis, and pupils were equal in size. Eye movements was normal but visual acuity in the right eye was 2/10 and in left 9/10. CT scan of the facial bones (slice thickness 1 mm) demonstrated a comminuted right orbital roof “blow-in” fracture (A,B,C,D) with associated non-displaced linear fracture extension towards the optic canal fracture. Magnetic resonance imaging MRI axial T2 flair showed a contusion of the right optic nerve (A,B,C,D). Traumatic optic neuropathy (TON) refers to optic nerve damage secondary to trauma, which occurs in approximately 0.5-5% of head injuries and 2.5% of patients with maxillofacial trauma and facial fractures. It is defined as any damage to the optic nerve secondary to trauma that may occur primarily or secondarily to the initial insult. It is crucial to make an appropriate diagnosis of orbital roof fracture if present because of its possible medical implications like enophthalmos or proptosis, facial asymmetry, visual loss, and eye movement restriction.
Figure 1: CT scan of the facial bones in axial plane (A), sagittal plane (B), and coronal plane (C) demonstrated a comminuted right orbital roof “blow-in” fracture, with associated non-displaced linear fracture extension towards the optic canal fracture. Magnetic resonance imaging MRI axial T2 flair (D) showed a contusion of the right optic nerve
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Article metrics
PlumX Metrics
Catastrophic optic canal fracture
