
Generalized granuloma annulare responsive to narrow band ultraviolet B therapy: case report and literature review
Khadija Elboukhari, Zakia Douhi, Sara Elloudi, Hanane Baybay, Fatima Zahra Mernissi
Corresponding author: Khadija Elboukhari, Department of Dermatology, University Hospital of Fez, Fez, Morocco 
Received: 02 Jan 2020 - Accepted: 15 Nov 2020 - Published: 18 Nov 2020
Domain: Dermatology
Keywords: Generalized, granuloma annulare, phototherapy
©Khadija Elboukhari et al. PAMJ Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Khadija Elboukhari et al. Generalized granuloma annulare responsive to narrow band ultraviolet B therapy: case report and literature review. PAMJ Clinical Medicine. 2020;4:106. [doi: 10.11604/pamj-cm.2020.4.106.21448]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com//content/article/4/106/full
Case report 

Generalized granuloma annulare responsive to narrow band ultraviolet B therapy: case report and literature review
Generalized granuloma annulare responsive to narrow band ultraviolet B therapy: case report and literature review
Khadija Elboukhari1,&, Zakia Douhi1, Sara Elloudi1, Hanane Baybay1, Fatima Zahra Mernissi1
&Corresponding author
Granuloma annulare (GA) is a rare, benign, inflammatory dermatosis of unknown origin, characterized by the annular arrangement of small papules. The generalized form is a very rare entity. It has been linked to several diseases, especially autoimmune thyroiditis. There is no established consensus for the treatment of generalized granuloma annulare but phototherapy is considered one of the best therapy options for this entity. We report a case of a 66-year-old woman, who presented this pathology, treated with phototherapy showing a good response.

Granuloma annulare is a rare benign inflammatory dermatosis, characterized by the annular arrangement of small papules. The generalized form is a very rare entity and is defined by the presence of more than 10 annular plaques or the presence of multiple plaques distributed over the trunk and limbs. Here we report the case of a woman who presented this disease, with a literature review.

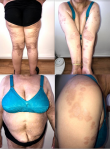
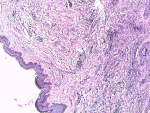
A 66-year-old woman, history of diabetes, presenting a general asymptomatic rash on the body evolving for two years, without regressive character, sensitive or sweating disorder. Physical examination showed multiple erythematous annular plaques with a paler center and an erythematous border localized at the ends and the trunk. Some lesions were slightly sclerotic (Figure 1). Many diagnoses were thought of including GA, Morphea, hypochromic fungal mycosis, parapsoriasis or borderline leprosy. When we put our dermoscope, we found diffuse whitish areas containing arborizing and linear vessels (Figure 2). Then, a skin biopsy was performed showing inflammatory charging dermis with densified collagen fibers (Figure 3), compatible with a generalized granuloma annulare in its incomplete interstitial form. The patient was treated with widespread narrow-band UVB phototherapy. After 35 sessions of (NB UVB) therapy, we noted a regression of the majority of lesions and the persistence of other localized lesions in hidden areas (Figure 4). Dermoscopy showed the persistence of some linear vessels with slight erythema (Figure 5). The patient is satisfied with the results and the treatment is still in progress. Apart from diabetes mellitus, the assessment of pathological associations did not show any anomalies.
This benign disease was first described in 1895 by Dr. Colcett Fox as a ringed eruption, then it has been nominated Granuloma annulare in 1992 by Dr. Radcliffe Crocker [1]. The localized form is the most frequent, occurring in 75% of reported cases and usually affecting the back of the hands and feet [2]. Although this benign inflammatory disease still has unclear causes, its histologic finding supports a delayed-type-T helper 1 cell-mediated hypersensitivity reaction [1]. Several associations have been reported such are autoimmune thyroiditis, HIV, EBV, viral hepatitis B infection, and malignancy. This latest association is still conflicted [3]. The link to diabetes mellitus has been recently rejected [4]. The generalized form of Granuloma annulare is a very rare entity that occurs in the elderly and is defined by the presence of more than 10 annular plaques or the presence of multiple plaques distributed over the trunk and limbs as was the case in our patient. It has a chronic relapsing evolution [5]. Differential diagnosis is essentially psoriasis in the annular form, tinea corporis, nummular eczema, pityriasis rosea, sarcoidosis, subacute lupus, necrobiosis lipoidica, and granulomatous mycosis fungoid [6]. In dermoscopic features, the whitish area with unfocused polymorphous vessels is the most common sign [7]. Histologically, GA is characterized by a necrobiosis or mucinous degradation of collagen that appears with a granulomatous type inflammation: palisading or interstitial histiocytes [8]. The abundant mucin is helpful to differentiate GA from the other infectious granuloma [9]. Therapeutically, GA is difficult to treat, particularly in the generalized form. In fact, there are no conclusive data in the management of GA. In the literature, we can only find case reports and small series [9]. The GGA is more difficult to treat, in this entity, lesions are more resistant to treatment. Phototherapy, especially Psoralen plus ultraviolet A (PUVA) therapy , is the most well studied therapeutic option for this variety, it should be used in the first-line therapy [10]. Narrow-band Ultraviolet B therapy is another alternative phototherapy with less risk of skin cancer. Although this therapy has been described as a successful treatment of GA [11,12], some other publications reported minimal to mild improvement [13], the case of our patient showed a good response. Other systemic therapies could be suggested in the second line, such are antimalarial, antibiotics like minocycline and fumarate acid esters. Biologic agents like tumor necrosis factor (TNF) alpha inhibitors have been reported as an efficient therapy of GA in some cases [14]. Corticosteroids can be effective, but there is a higher risk of recurrence when stopped [14,15].
Generalized granuloma annulare is a benign affection characterized by a chronic evolution and the difficulties of treatment. First-line therapy is phototherapy. NB-UVB finds its place in this pathology.
The authors declare no competing interests.
All authors contributed to the conduct of this work. They have read and approved the final version of the manuscript.
We are indebted to the patient for giving us the consent for the publication.
Figure 1: diffuse erythematous annular plaques of the trunk and limbs
Figure 2: whitish area with linear vessels seen by dermoscopy
Figure 3: HES
coloring G x 50. Inflammatory charged dermis + densified collagen fibers
Figure 4:
attenuation of lesions after NB-UVB therapy, especially in the trunk with the
persistence of annular lesions in hidden locations
Figure 5: dissolve of the whitish area with persistent slight erythema seen in dermoscopic control
- Little EG. Granuloma annulare. Proc R Soc.Med. 1908;1:95-163.
- Cyr PR. Diagnosis and management of granuloma annulare. AFP. 2006 Nov 15;74(10):1729-34. PubMed | Google Scholar
- Mestre T, Rodrigues AM, Cardoso J. Disseminated granuloma annulare and hepatocellular carcinoma: association or coincidence. BMJ Case Rep. 2014 Oct 28;2014:bcr2014205883. PubMed | Google Scholar
- Nebesio CL, Lewis C, Chuang TY. Lack of an association between granuloma annulare and type 2 diabetes mellitus. Br J Dermatol. 2002 Jan;146(1):122-4. PubMed | Google Scholar
- Gabaldón VH, Haro-González-Vico V. Lack of an association between generalized granuloma annulare and malignancy: a case-control study. J. Am. Acad. Dermatol. 2019 Jun;80(6):1799-1800. PubMed | Google Scholar
- Thornsberry LA, English JC. Etiology, diagnosis, and therapeutic management of granuloma annulare: an update. Am J Clin Dermatol. 2013 Aug;14(4):279-90. PubMed | Google Scholar
- Yun JH, Lee JY, Kim MK, Seo YJ, Kim MH, Cho KH et al. Clinical and pathological features of generalized granuloma annulare with their Correlation: a retrospective multicenter study in Korea. Ann Dermatol. 2009 May;21(2):113-9. PubMed | Google Scholar
- Errichetti E, Lallas A, Apalla Z, Di Stefani A, Stinco G. Dermoscopy of Granuloma annulare: a clinical and histological correlation study. Dermatology. 2017;233(1):74-79 PubMed | Google Scholar
- Scuola Dermatologica Chimenti. Granuloma annulare disseminato non responsivo alle comuni terapie immunosoppressive: l´utilizzo dell´anti-tnf come alternativa terapeutica. Accessed January 3 2020.
- Browne F, Turner D, Goulden V. Psoralen and ultraviolet A in the treatment of granuloma annulare: PUVA in the treatment of granuloma annulare. Photodermatology, Photoimmunology & Photomedicine. 2011 Apr;27(2):81-4. PubMed | Google Scholar
- MDedge Dermatology. Generalized Granuloma Annulare Responsive to Narrowband UVB. Accessed January 3 2020.
- Inui S, Nishida Y, Itami S, Katayama I. Disseminated granuloma annulare responsive to narrowband ultraviolet B therapy. Journal of the American Academy of Dermatology. 2005 Sep;53(3):533-4. PubMed | Google Scholar
- Samson Yashar S, Gielczyk R, Scherschun L, Lim HW. Narrow-band ultraviolet B treatment for vitiligo, pruritus, and inflammatory dermatoses. Photoderm Photoimm Photomed. 2003 Aug;19(4):164-8. PubMed | Google Scholar
- Kozic H, Webster GF. Treatment of Widespread granuloma annulare with Adalimumab. J Clin Aesthet Dermatol. 2011 Nov;4(11):42-3. PubMed | Google Scholar
- Queue. Perforating granuloma annulare: a case report and literature review. Accessed January 3 2020.
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures



Article metrics

