
Reversible hyperpigmentation in Vitamin B12 deficiency: an Addisonian mimic in clinical practice
Rosemary Abena Kuenyefu Awindaogo, Ivy Ekem, Nana Agyeiwah Awuku, Soziema Salia, Martin Agyei, Yvonne Ayerki Nartey, Yaw Asante Awuku
Corresponding author: Rosemary Abena Kuenyefu Awindaogo, Department of Internal Medicine, Cape Coast Teaching Hospital, Cape Coast, Ghana 
Received: 23 Oct 2020 - Accepted: 12 Nov 2020 - Published: 19 Nov 2020
Domain: Internal medicine
Keywords: Hyperpigmentation, vitamin B12 deficiency, helicobacter pylori, gastritis
©Rosemary Abena Kuenyefu Awindaogo et al. PAMJ Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Rosemary Abena Kuenyefu Awindaogo et al. Reversible hyperpigmentation in Vitamin B12 deficiency: an Addisonian mimic in clinical practice. PAMJ Clinical Medicine. 2020;4:109. [doi: 10.11604/pamj-cm.2020.4.109.26641]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com//content/article/4/109/full
Case report 

Reversible hyperpigmentation in Vitamin B12 deficiency: an Addisonian mimic in clinical practice
Reversible hyperpigmentation in Vitamin B12 deficiency: an Addisonian mimic in clinical practice
.gif) Rosemary Abena Kuenyefu Awindaogo1,&, Ivy Ekem2, Nana Agyeiwah Awuku3, Soziema Salia1, Martin Agyei4, Yvonne Ayerki Nartey1, Yaw Asante Awuku1
Rosemary Abena Kuenyefu Awindaogo1,&, Ivy Ekem2, Nana Agyeiwah Awuku3, Soziema Salia1, Martin Agyei4, Yvonne Ayerki Nartey1, Yaw Asante Awuku1
&Corresponding author
Vitamin B12 deficiency may present with gastrointestinal, haematologic, dermatologic and neuropsychiatric signs and symptoms. Skin hyperpigmentation is a dermatologic manifestation which may mimic the features seen in Addison´s disease. We report a case of a 33-year-old non-vegan man who presented with progressive darkening of his palms, knuckles and feet which was associated with anaemia. Low serum vitamin B12 levels coupled with characteristic morphology of peripheral blood smear and bone marrow aspirate were identified. An extensive work up to establish the cause of Vitamin B12 deficiency revealed Helicobacter pylori associated gastritis as the likely aetiology. The patient had significant reversibility of hyperpigmentation and normalisation of the haematological indices following parenteral vitamin B12 supplementation. This case highlights the need for a high index of suspicion when clinicians are faced with a case of hyperpigmentation, so that the appropriate treatment can be promptly instituted and the late irreversible complications of vitamin B12 deficiency prevented.

Vitamin B12 (cobalamin), is a water soluble and cobalt containing vitamin present in meat, poultry and dairy products. It cannot be synthesised in the human body and consequently is obtained by humans solely through their diet. Deficiency is relatively uncommon, due to the presence of body stores which may last for up to 5 years [1]. Hyperpigmentation as a clue to the diagnosis of systemic diseases is associated with multiple aetiologies. The pattern of pigmentation in vitamin B12 deficiency may sometimes be confused with, or mimic Addison´s disease. It is therefore important for clinicians to take a detailed clinical history and conduct a thorough physical examination, in order to tailor diagnostic tests and treatments accordingly. We report a case of vitamin B12 deficiency with reversible palmoplantar hyperpigmentation that was initially suspected to be Addison´s disease. The patient was found to have vitamin B12 deficiency secondary to H. pylori associated gastritis and had reversal of the hyperpigmentation following parenteral vitamin B12 supplementation.

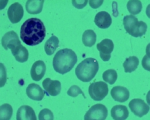
A 33-year-old non-vegan male patient presented with a one-year history of progressive darkening of his palms. He initially attributed his symptoms to regular handling of money due to his occupation as a banker, however his symptoms gradually progressed to involve the knuckles and both soles of his feet. Associated symptoms included anorexia, dysgeusia, easy fatiguability and dizziness. He also noticed 20kg weight loss over the 2 months prior to his presentation. With regard to his past medical history, he had received 2 units of whole blood on account of symptomatic anaemia 5 months prior to presentation at our health facility. He had no known chronic illnesses, was on no medications and had no previous gastrointestinal (GI) surgeries. His family and social histories were unremarkable, and there were no dietary restrictions reported. On examination, he was moderately pale, anicteric, with normal buccal mucosa and tongue. Hyperpigmentation involving palms of both hands, knuckles of all fingers, pre-auricular skin, lips and soles of both feet were noted. Darkening of both palms were uniform with no accentuation of the palmer creases while those of the planter skin was non-uniform and accentuated in the instep. The hair, nails and other mucosal surfaces were normal. Neurologic and all other systemic examination were unremarkable. Complete blood count (CBC) showed a macrocytic anaemia with an Hb of 5.9g/dl and mean cell volume (MCV) of 102.2fl. White blood cell (WBC) and Platelet counts were normal as well as renal and liver function tests. There was an initial clinical suspicion for Addison´s disease, possibly secondary to a malignancy, because the patient had experienced dramatic weight loss of 20kg in a period of just 2 months, however serum cortisol and Adrenocorticotropic hormone (ACTH) performed were within normal limits. A peripheral blood smear demonstrated anisopoikilocytosis with moderate hyperchromia, multiple hypersegmented neutrophils and eosinophilia. A similar picture of hypersegmented neutrophils was described by Professor Ivy Ekem in 2009 [2] (Figure 1). Platelets were adequate with normal morphology. Serum folate assay was normal at 26.3nmol/L (4.56 - 45.4nmol/L), and serum vitamin B12 level was low at 101.2pmol/L (normal >147pmol/L).
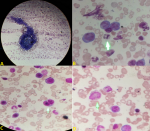
Bone marrow aspirate revealed hypercellular fragments and trails, hyperplastic red cells with megaloblasts and dyserythropoeitic forms (Figure 2). There was also active granulopoeisis with a disproportionate number of eosinophils and evidence of poor maturation, especially in the myelocyte cell lines. Additionally, hypersegmented neutrophils were evident and megakaryocytes had polyploid nuclei. The lymphocytes present showed some immaturity in the nuclei, and the plasma cells and macrophages present were normal. A diagnosis of hyperpigmentation secondary to vitamin B12 deficiency was therefore made, however the cause of the vitamin B12 deficiency was not immediately evident. Consequently, serum antibodies to parietal cells and intrinsic factor were requested and found to be negative, ruling out pernicious anaemia. CT scan of the abdomen with barium follow through to determine ileal integrity was also normal. Stool examination for ova and parasites were likewise negative. Oesophagogastroduodenoscopy demonstrated mild atrophic changes in the stomach with a positive urease test, indicative of Helicobacter pylori infection. Histopathology of multiple gastric biopsies taken during endoscopy revealed non-specific inflammation of the gastric mucosa. A definitive diagnosis of vitamin B12 deficiency secondary to H. pylori associated gastritis was therefore made. The patient was started on intramuscular (IM) vitamin B12 1,000 mcg three times weekly for one month, then monthly for the subsequent three months. He was also started concurrently on H. pylori eradication therapy with clarithromycin 500mg twice daily, amoxicillin 1g twice daily and omeprazole 20mg twice daily all for 14 days. Within the first two weeks of therapy, hyperpigmentation improved significantly and his haematological profile almost approached normal as shown in Table 1. Following completion of three months of IM vitamin B12 injections, the serum Vitamin B12 assay normalised to a value of 429.2pmol/L (normal >147pmol/L) with a progressive improvement of the palmar and plantar hyperpigmentation (Figure 3, Figure 4).
The differential diagnoses for cutaneous hyperpigmentation include a myriad of clinical conditions which may be due to normal variants, congenital or inherited disorders and finally, acquired conditions. The cornerstone of successful diagnosis and management includes a detailed medical history and thorough examination, which in turn informs the clinician of the required work-up for a definitive diagnosis. Acquired causes of hyperpigmentation include but are not limited to excessive sun exposure, medications, endocrine and disorders such as Addison´s disease and nutritional causes such as vitamin B12 deficiency [3]. As far back as September 1944, Dr Bramwell Cook described a vitamin B12 deficiency syndrome characterised by macrocytic anaemia, glossitis and hyperpigmentation of the skin [4]. Indeed, it is well described that the presence of vitamin B12 deficiency may be associated with a multitude of mucocutaneous manifestations including vitiligo, hair changes, glossitis and hyperpigmentation which may involve creases of the palms and soles, oral mucosa, dorsum of the hands and feet and angular stomatitis [1,5,6]. It has been shown that up to one in five affected patients may present with cutaneous hyperpigmentation [1], therefore it is not unusual that this patient had hyperpigmentation as one of his primary clinical features. The mechanism of hyperpigmentation is poorly understood but it is thought to be related to increased melanin synthesis rather than a defect in melanin [6]. Further studies on the pathophysiology of hyperpigmentation in B12 deficiency would therefore be informative.
The prevalence of vitamin B12 deficiency in Ghana is not well characterized, however one national level survey found a prevalence of 6.9% among non-pregnant females [7], and another study in the Ashanti region reported a prevalence of 30% among apparently healthy adults [8]. Of note is the increased prevalence of anaemia among individuals with lower educational and socioeconomic status [8], and it was therefore interesting to discover vitamin B12 deficiency in this middle class patient with no dietary restriction. Moreover, as published in a case series by Ekem in 2009, and additionally demonstrated in a study conducted in Zimbabwe, such significant deficiency is more likely to be found in female patients [2,9]. Such presentation in a male patient was certainly uncommon in our clinical experience, and the patient was therefore worked up further for the cause of his vitamin B12 deficiency. Causes of vitamin B12 deficiency include pernicious anaemia, inadequate dietary intake, post-GI surgery, atrophic gastritis and H. pylori infection. Following exclusion of other causes, upper GI endoscopy with subsequent gastric biopsy demonstrated H. Pylori associated gastritis as the likely cause of his deficiency. The cause of cobalamin deficiency from H. Pylori associated gastritis is not clear but it has been postulated that inflammation of the gastric mucosa can lead to B12 disintegration from food binders. H. Pylori infection was reportedly associated with approximately half of all patients with cobalamin deficiency in a study by Kaptan et al. [10]. It has also been suggested that eradication of H. Pylori alone may restore cobalamin levels and correct B12 deficiency, therefore the importance of H. pylori eradication therapy cannot be understated.
Hyperpigmentation is an early and reversible sign of vitamin B 12 deficiency, which must be promptly recognised and corrected. The cause of B12 deficiency must be identified and additionally treated. Clinicians should have a broad differential diagnosis for palmoplantar hyperpigmentation that includes B12 deficiency, so that investigations are properly directed and the patient adequately managed.
The authors declare no competing interests.
This work was carried out in collaboration with all authors. Author YAA and RAKA were involved in clinical care, conceptualization and collection of data. Authors RAKA and YAN were responsible for drafting the manuscript. Authors NAA, IE, MA, and SS were involved in clinical care of the patient, and editing and reviewing the manuscript. All authors read and approved the final manuscript.
We express our profound appreciation to Dr Felicia Amihere for her assistance in managing the patient, Dr Ampem Darko Siaw Jr. and Dr. Kofi Abankroh in the production of the manuscript.
Table 1: complete blood count parameters over the treatment period
Figure 1: blood film comment showing a hypersegmented neutrophil seen in a similar case by Ekem in 2009
Figure 2: bone marrow aspirate demonstrating A) hypercellular fragment with trail; B) megaloblasts surrounding hypersegmented neutrophil; C) dysplastic erythroblast; D) giant metamyelocyte
Figure 3: palms at initial
presentation; one month to 3 months post-treatment
Figure 4: soles at initial
presentation; one month to 3 months post-treatment
- Aaron S, Kumar S, Vijayan J, Jacob J, Alexander M, Gnanamuthu C. Clinical and laboratory features and response to treatment in patients presenting with vitamin B12 deficiency-related neurological syndromes. Neurology India. 2005;53(1):55. PubMed | Google Scholar
- Ekem IA. Hypersegmented neutrophils and reversible hyperpigmentation in vitamin B12 deficiency in Ghana. BMJ Case Reports. 2009;2009:bcr0820080686. PubMed | Google Scholar
- Vashi N, Kundu R. Acquired hyperpigmentation disorders. UpToDate. 2017.
- Cook A. A vitamin B deficiency syndrome allied to sprue. The Indian Medical Gazette. 1944;79(9):429. PubMed | Google Scholar
- Kannan R, Ng M. Cutaneous lesions and vitamin B12 deficiency: an often-forgotten link. Canadian Family Physician. 2008;54(4):529-532. PubMed | Google Scholar
- Cherqaoui R, Husain M, Madduri S, Okolie P, Nunlee-Bland G, Williams J. A reversible cause of skin hyperpigmentation and postural hypotension. Case reports in hematology. 2013;2013:680459. PubMed | Google Scholar
- Wegmüller R, Bentil H, Wirth JP, Petry N, Tanumihardjo SA, Allen L et al. Anemia, micronutrient deficiencies, malaria, hemoglobinopathies and malnutrition in young children and non-pregnant women in Ghana: findings from a national survey. PloS one. 2020;15(1):e0228258. PubMed | Google Scholar
- Owiredu W, Kotey A, Laing E, Frempong M, Abledu J, Amidu N et al. Haemato-biochemical basis of anaemia in Agogo, Ashanti Region, Ghana. Journal of Medical and Biomedical Sciences. 2016;5(3):1-12. Google Scholar
- Savage D, Gangaidzo I, Lindenbaum J, Kiire C, Mukiibi JM, Moyo A et al. Vitamin B12 deficiency is the primary cause of megaloblastic anaemia in Zimbabwe. British journal of haematology. 1994;86(4):844-850. PubMed | Google Scholar
- Kaptan K, Beyan C, Ural AU, Cetin T, Avcu F, Gülşen M et al. Helicobacter pylori - is it a novel causative agent in vitamin B12 deficiency. Archives of Internal Medicine. 2000;160(9):1349-1353. PubMed | Google Scholar
Search

This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures


Article metrics
Recently from the PAMJ-CM






