
Giant unruptured intracranial aneurysm
Hassan Baallal, Hatim Belfquih
Corresponding author: Hassan Baallal, Department of Neurosurgery, Avicenne Military Teaching Hospital, University Caddi Ayyad, Marrakech, Morocco 
Received: 28 Aug 2020 - Accepted: 16 Sep 2020 - Published: 25 Sep 2020
Domain: Neurosurgery,Vascular surgery
Keywords: Intracranial aneurysms, endovascular coiling
©Hassan Baallal et al. PAMJ Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Hassan Baallal et al. Giant unruptured intracranial aneurysm. PAMJ Clinical Medicine. 2020;4:39. [doi: 10.11604/pamj-cm.2020.4.39.25796]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com//content/article/4/39/full
Images in clinical medicine 

Giant unruptured intracranial aneurysm
Giant unruptured intracranial aneurysm
Hassan Baallal1,&, Hatim Belfquih1
&Corresponding author

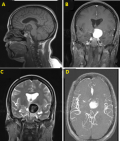
Giant intracranial aneurysms (GIAs) are rare and heterogeneous lesions with complex vascular anatomy and represent almost 5% of intracranial aneurysms. The formation and growth of an aneurysm is the result of a complex interaction of multiple factors. In addition to genetic, physiological, environmental factors, and tissue mechanics, it is believed that fluid dynamics play an important role in the formation and development of arterial aneurysms at certain sites. The majority of the brain aneurysms are observed at bifurcations or arterial branches located in the circle of Willis where the flow topology is complex. In this report, we present a 55-year-old woman patient who was referred to our neurosurgical department with a three years history of an intermittent holocephalic headache, beginning cognitive deficits and lethargy magnetic resonance imaging (MRI) obtained from the referring hospital reported supra-sellar mass, 55 mm in diameter with a crescent shaped hypo-intensity of the lesion wall in the T1-weighted frame (A) and T2 -weighted frame (A, B), with enhancement of the lesion wall and intraluminal flow void after administration of gadolinium (C,D). Exploration of the supra-aortic arteries was normal. No other sources of brain infarction were found on electrocardiogram, transthoracic echocardiography and Holter monitoring. The patient was referred to interventional neuroradiology for endovascular coiling of the aneurysm.
Figure 1: magnetic resonance imaging (MRI) obtained from the referring hospital reported supra-sellar mass, 55 mm in diameter with a crescent shaped hypo-intensity of the lesion wall in the T1-weighted frame and T2 -weighted frame (A, B), with enhancement of the lesion wall and intraluminal flow void after administration of gadolinium (C,D)
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Article metrics
PlumX Metrics
Giant unruptured intracranial aneurysm
