
Spontaneous rupture of the renal pelvis in a teenager: case report
Youness Chakir, Yassine Rachid, Mohamed Dakir, Adil Debbagh, Rachid Aboutaieb
Corresponding author: Youness Chakir, Ibn Rochd UHC, Casablanca, Morocco 
Received: 29 Dec 2019 - Accepted: 02 Nov 2020 - Published: 02 Nov 2020
Domain: Urology
Keywords: Urinoma, derivation, spontaneous
©Youness Chakir et al. PAMJ Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Youness Chakir et al. Spontaneous rupture of the renal pelvis in a teenager: case report. PAMJ Clinical Medicine. 2020;4:74. [doi: 10.11604/pamj-cm.2020.4.74.21362]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com//content/article/4/74/full
Case report 

Spontaneous rupture of the renal pelvis in a teenager: case report
Spontaneous rupture of the renal pelvis in a teenager: case report
Youness Chakir1,&, Yassine Rachid1, Mohamed Dakir1, Adil Debbagh, Rachid Aboutaieb1
&Corresponding author
We report a case of a 15-year-old Moroccan boy, with a perinephric urinoma, whose health had previously been good, but who experienced a sudden onset of right flank pain. Radiological examination: right kidney increased in size, poorly differentiated with bumpy contours with bad rotation, major ureterohydronephrosis laminating the cortex, late contrast extravasation in the perirenal to the pelvis. Double JJ drainage was performed without incident. Urinoma is a rare complication of obstruction of the urinary tract, and it occurs most commonly following renal trauma, in our case we have not found any clear reason to explain the etiology of obstruction and extravasation, but we put etiological assumptions.

Spontaneous rupture of the urinary excretory system is a rare condition. It is mainly associated with obstruction of the excretory system and is usually unilateral, in some cases we do not found a reason, management initially remains conservative under close follow up [1].

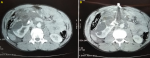
M.E, aged 15, with no particular pathological history. The reason for hospitalization: spontaneous right flank pain on a malformed right kidney, its history of his pain dates back to 24 hours before admission by the occurrence in the right lumbar fossa of abdominal pain diffuse and vomiting, in a context of febrile sensations and diuresis preserved without notion of gross hematuria. Physical examination showed knocking tenderness over the right costovertebral angle. Paraclinical examination showed: Hb: 13.3 g/dl, creatinine: 9mg/L, GB: 26790elts\mm3, platelets:120000elts\mm3, CRP: 6mg\dl and correct hemostasis assessment. The findings of the urine analysis were as follows: leukocyte count, 0-1/ high-power field (HPF); erythrocyte count, 6/HPF; nitrite (-); leukocyte esterase (-); protein (-); and occult blood (-). Abdominal ultrasound showed a moderate right uretero hydronephrosis (UHN) with finely echogenic content, peritoneal effusion to the right iliac fossa. Pelvic abdominal CT, Figure 1 showed a right kidney enlarged in size of bumpy contours poorly differentiated badly rotated, major uretero hydronephrosis laminating the cortex, calculation in medio renal of 10 mm, density: 1150 Hounsfield Unit (HU), significant enhancement of the pyelo-ureteral wall, urinary extravasation in peri-renal to the pelvis, large abundance of retro-peritoneal and intra-peritoneal effusion, multiple lumbo-aortic, mesenteric and external iliac lymphadenopathies.
The spontaneous rupture of the pyelocalicial excretory system is a rare entity that can have significant clinical repercussions, and is defined as extravasation of urine into the perirenal tissue and retroperitoneum in the absence of inflammation, trauma, prior instrumentation, surgery or kidney disease. Almost all of them are associated with obstruction of the excretory system, mainly lithiasis and less frequent causes such as stenosis, trauma, tumor or connective tissue disease [1]. There are a number of reports on spontaneous extravasation of urine from the renal pelvis and ureter but many are isolated case reports [2]. Spontaneous rupture of the ureter was first reported by Albarran in 1895. In 1952 Orkin reviewed 26 cases, Shaw et al. (1957) collected 40 case reports of spontaneous rupture of the kidney and all but 3 of these were hydronephrotic. In half of these cases the tear was through the pelvis and in the remainder it was through the renal parenchyma [3]. Clinically, it manifests as sudden, intense low back pain, sometimes simulating an acute abdomen, with nausea and vomiting like renal colic, or even simulating acute cholecystitis or appendicitis [1]. From the classic descriptions of elimination pyelography and computed tomography (CT), imaging diagnosis is essential to determine its location, amount, presence of complications and evolution [1].
In a recent prospective observational high volume single center study of spontaneous upper urinary tract rupture (s-UUTR): out of 1629 patients admitted to the emergency department, for renal colic and studied by kidney ultrasound and contrast enhanced CT (CECT), 31 patients had a spontaneous s-UUTR. Presentation, therapeutic procedures and outcomes were registered. The stone was most commonly identified at the vesicoureteric junction (VUJ) (61.3%) and mean stone size was 5.71 mm. S-UUTR was most frequently located in a calyx (54.84%). Twenty-six patients (83.87%) had a clinical presentation of a renal colic, 3 cases (9.68%) had an atypical presentation and 2 (6.45%) presented an acute abdomen. Our patient had a sudden onset of right flank pain and in CT, we identified a medial calyx stone of 10mm. In 26 cases a J-J stent (83.87%) was placed, 3 patients underwent primary ureteroscopic lithotripsy (9.67%); in 1 patient (3.23%) a nephrostomy was inserted and in 1 case (3.23%) active surveillance was adopted. Cases who underwent sole urinary derivation were revaluated after 30 days: ureteroscopic lithotripsy was performed in 48.15% of the cases; extracorporeal shock wave lithotripsy in 3.7%; in 22.2% of cases a CT demonstrated the spontaneous expulsion of the stone. The patient undergoing an active surveillance spontaneously expelled the stone. In this result experience, most patients were actively treated with good results but a conservative approach can be offered in selected cases. In our experience, a double J was placed, neither uretereroscopy nor lithotripsy was performed and he did not expulse any stone.
The most common location of rupture, is at the fornix point of greatest weakness at increased intraluminal pressure. Their association with obstructive pathology which considerably increases the intraluminal pressure, most often secondary to an impacted lithiasis. In the vast majority of cases, it is unilateral. Less common causes are tumors, pregnancy, posterior urethral leaflets, retroperitoneal fibrosis and, pelviureteric junction or vesicoureteric junction obstruction. Some cases have also been reported in association with knotty periarteritis, dermatomyositis and lupus, ovarian tumor, bilateral rupture during a pyelography or CT urography are reported [1,4]. Some authors reported other causes, enlarged lymphatic glands, ruptured renal cysts, postradiation scars, renal transplants and enlarged prostate gland [4]. In some cases no cause is found and the etiology of extravasation remained unclear in the other cases [4]. In our case the etiology remains unclair. Pajaneen et al. in eight patients with sudden onset of flank pain, urography showed extravasation of urine. The cause of peripelvic leakage was verified ureteral stone in four cases, stricture of the ureteropelvic junction in one, and unknown in three cases. Treatment was symptomatic in four cases; drainage in two and surgery in two cases. Seven patients recovered uneventfully, but one required nephrectomy. The prognosis in spontaneous urinary extravasation is usually good without drainage. Open surgery is seldom indicated [4].
Urinomas are common after renal trauma or perforation of the collecting system during an endo surgical procedure. Perirenal urine extravasation is a rare complication of congenital obstruction of the urinary tract. In more than 70% of children, perirenal urinomas and urinary ascites are associated with the posterior urethral valves. Other reported pathologies are uretero pyelocaliceal junction obstruction (UPJ-O), ureteral valves, ureterocele, urethral atresia, bladder neck obstruction in conjunction with reflux, and sometimes without any evidence of obstructive uropathy like our patient. UPJ-O is the most common obstructive lesion in childhood, and congenital abnormalities are the most common cause of this condition in young children. In older children, UPJ-O may be caused by compression of the ureter, inflammation, retroperitoneal fibrosis, kidney stones, or scar tissue from previous surgery to correct the UPJ-O. Over 90% of patients with urinoma due to obstructive uropathy are successfully treated by percutaneous drainage to relieve the obstruction [5]. Our patient had no history of renal trauma, he had not undergone any surgical procedure in the past, and he had no history of urinary tract infection or it has no history of urolithiasis emission. The urinoma may have been spontaneous and secondary to congenital or lithiasis obstruction, as a result of increased transmitted back pressure or renal intrapelvic pressure, but the actual cause of his condition remains unclear.
Contrast-enhanced imaging studies are not recommended as the first-line imaging methods for the evaluation of patients with acute flank pain and clinically insignificant ruptures are probably left diagnosed. Contrast-enhanced CT with nonenhanced images is the most sensitive and specific noninvasive imaging modality. Laminar fluid collection in perirenal space in patients with renal colic is probably underreported by radiologists, and this finding is usually not associated with significant clinical consequences. Serial ultrasound evaluations show a high sensitivity for detecting a small amount of fluid extravasation but a low specificity for distinguishing urinoma from hematoma or abscess. Quantification of urine extravasation was classified in two grades. Fluid collection in proximity to the pelvicalyceal system, and small amount of perirenal extravasation mainly limited around the lower renal pole is classified as grade 1. Large fluid collection in perinephric area with expansion in the retroperitoneum is classified as grade 2. According to this urine extravasation grading system, our patient can be classified as grade 2. Retrograde pyelography can also be used in patients whose diagnosis is left uncertain with other imaging methods. Intravenous pyelogram is a very sensitive and specific method to confirm the diagnosis of urine extravasation [6]
In our case ultrasonography showed a moderate right uretero hydronephrosis UHN with finely echogenic content, peritoneal effusion to the right iliac fossa. CT showed major uretero hydronephrosis laminating the cortex, a lithiasis in medio renal calyx of 10 mm, 1150 Hounsfield Unit (HU), significant enhancement of the pyelo-ureteral wall, a perirenal urinary extravasation to the pelvis, large abundance of retro-peritoneal and intra-peritoneal effusion, multiple lumbo-aortic, mesenteric and external iliac lymphadenopathies. Our patient had a malrotated kidney, and we can pose as hypothesis on the cause of the obstruction, the calculus which was found in mid renal, we supposed that it migrated during the extravasation of the urine, also we can assume that the etiology of the obstruction is due to lumboaortic lymphadenopathy. We derived our patient by a double J stent, without incident, the clinical course was marked by the disappearance of febrile sensations and the hemodynamic state which remained stable, the double J stent was removed at three months of follow-up.
The spontaneous rupture of the pyelocalicial excretory system is rare, can have serious problems and early urinary diversion with a stent prevents complications.
The authors declare no competing interests.
All authors managed the patient, C.Y wrote the article. All the authors have read and agreed to the final manuscript.
Figure 1: pelvic abdominal CT, showed a right kidney enlarged in size with major ureterohydronephrosis laminating the cortex, with urinoma
- Miranda R, Latorre P, Raurich R. Ruptura pieloureteral espontánea bilateral durante un urotac: caso clínico. Rev méd Chile. avr 2017;145(4):544-8. Google Scholar
- Spinelli MG, Palmisano F, Zanetti SP, Boeri L, Gadda F, Talso M et al. Spontaneous upper urinary tract rupture caused by ureteric stones: a prospective high-volume single centre observational study and proposed management. Arch Esp Urol. juill 2019;72(6):590-5. PubMed | Google Scholar
- Ramsey EW, Jarzylo SV, Bruce AW. Spontaneous extravasation of urine from the renal pelvis and ureter. Journal of Urology. nov 1973;110(5):507-12. PubMed | Google Scholar
- Paajanen H, Kettunen J, Tainio H, Jauhiainen K. Spontaneous peripelvic extravasation of urine as a cause of acute abdomen. Scandinavian Journal of Urology and Nephrology. Sept 1993;27(3):333-6. PubMed | Google Scholar
- Tseng P-C, Liu T-Y, Pan S-J, Sung D-S. Spontaneous perirenal urinoma associated with ureteropelvic junction obstruction in a child: a case report. Pediatrics & Neonatology. June 2009;50(3):121-4. PubMed | Google Scholar
- Yanaral F, Ozkan A, Cilesiz N, Nuhoglu B. Spontaneous rupture of the renal pelvis due to obstruction of pelviureteric junction by renal stone: a case report and review of the literature. Urol Ann. 2017;9(3):293. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures
Article metrics

