
Acute abdomen revealing torsion of intra-abdominal testicular seminoma: a case report
Houssame Lachhab, Adil Kbirou, Mehdi Safieddine, Yassine Daghdagh, Mohammed Dakir, Adil Debbagh, Rachid Aboutaieb, Yassine Harmoumi, Najwa Touil, Omar Kacimi, Abdellatif Siwane, Houria Tabakh, Nabil Chikhaoui
Corresponding author: Houssame Lachhab, Department of Urology, Ibn Rochd University Hospital, Casablanca, Maroc 
Received: 06 Jun 2020 - Accepted: 18 Jan 2021 - Published: 21 Jan 2021
Domain: Urology
Keywords: Testicular torsion, intra-abdominal testis, cryptorchidism, seminoma
©Houssame Lachhab et al. PAMJ Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Houssame Lachhab et al. Acute abdomen revealing torsion of intra-abdominal testicular seminoma: a case report. PAMJ Clinical Medicine. 2021;5:28. [doi: 10.11604/pamj-cm.2021.5.28.24091]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com//content/article/5/28/full
Case report 

Acute abdomen revealing torsion of intra-abdominal testicular seminoma: a case report
Acute abdomen revealing torsion of intra-abdominal testicular seminoma: a case report
![]() Houssame Lachhab1,&, Adil Kbirou1, Mehdi Safieddine1, Yassine Daghdagh1, Mohammed Dakir1, Adil Debbagh1,, Rachid Aboutaieb1, Yassine Harmoumi2, Najwa Touil2, Omar Kacimi2, Abdellatif Siwane2, Houria Tabakh2, Nabil Chikhaoui2
Houssame Lachhab1,&, Adil Kbirou1, Mehdi Safieddine1, Yassine Daghdagh1, Mohammed Dakir1, Adil Debbagh1,, Rachid Aboutaieb1, Yassine Harmoumi2, Najwa Touil2, Omar Kacimi2, Abdellatif Siwane2, Houria Tabakh2, Nabil Chikhaoui2
&Corresponding author
Testicular seminoma is the most common malignant tumor of the testis. The risk of developing cancer is higher if the testis is not descended. However, torsion of a neoplastic intra-abdominal testis is a very rare clinical condition, which is not normally considered in the differential diagnosis of acute abdomen. A case of intra-abdominal torsion of a malignant testicular tumor is reported.

The incidence of testicular cancer has continued to rise in recent decades. In 2006, approximately 8,250 new cases of testicular germ cell tumors were diagnosed in the USA. The increased risk associated with cryptorchidism is particularly significant. Approximately 10% of testicular tumors are associated with cryptorchidism. The malignant transformation of a cryptorchid testis occurs 3 to 14 times more often than a normal testis [1]. Such a testis is also vulnerable to torsion due to rapid increase in tumor size and free mobility. The clinical presentation suggests an acute abdomen [2].

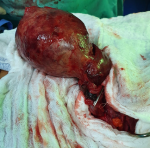
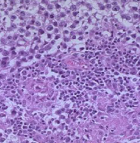
An 18-year-old male presented to our hospital 3 days after developing an acute left lower quadrant pain accompanied by bouts of vomiting and a low-grade fever. He had a pulse rate of 82/min and blood pressure of 120/60 mmHg. His abdominal examination revealed a tenderness and a bulging mass of the left iliac fossa reaching the navel. The left testicle was absent from the scrotal sac. Biological examinations were within normal limits with a white blood cell count of 10770/cumm, tumor markers also normal (alpha-fetoprotein = 1,3 ng/ml, HCG <1.20 UI/l) except for LDH (= 670 UI/L). Emergency pelvi-abdominal U/S showed a hypogastric mass lateralized to the left. An abdominal CT Scan with contrast (Figure 1) was then performed which revealed a well-defined hypodense mass 9 x 8.2 x 6.3cm in size arising from left side of the pelvis, extending superior and anterior to the bladder. Exploratory laparotomy was performed through a midline incision which revealed a large 9.5 x 9 x 6 cm well-capsulated mass, torted 360º on its pedicle counterclockwise (Figure 2). The pedicle was clamped, and the mass was removed (Figure 3). Formal abdominal exploration was done, and no evidence of suspicious lymph nodes or other masses was found. The mass weighed 308g. The specimen was sent for histopathological examination. Histopathology report was seminoma with features of round to polyhedral cells arranged in sheets and trabeculae separated by septae traversed by lymphocytes (Figure 4). The stroma showed extensive areas of necrosis with no peri-capsular infiltration. Later, the patient completes his course of treatment with the oncology department in our hospital.
The relative risk of testicular cancer on cryptorchidism, long estimated at nearly 40 compared to populations with no history of cryptorchidism, is estimated between 2.75 and 8. If we exclude populations at risk particular (genetic syndromes and other conditions predisposing), the relative risk for a man who had an isolated cryptorchidism can be evaluated at 2.9 [3]. The most serious complications of cryptorchidism, which are extensively discussed in the literature, are a high rate of infertility and a high incidence of testicular cancer. Early surgical intervention in cryptorchidism is currently aimed at preserving germinal epithelium, decreasing the rate of infertility, and situating the testis in a position that allows better access for self-physical examination and earlier detection of testicular cancer [4]. Pure seminoma represents more than 90% of the histopathological features of undescended testicular tumors in adulthood [5]. Five to ten percent of testicular tumors occur in the contralateral, normally descended testis [2]. Orchiopexy is ideally performed prior to the first year of age with the intent of preventing these issues. Gaudio et al. demonstrated the decrease of germ cell density in cryptorchidism after 1 year of age. However, management with orchiopexy has not been proven for risk reduction of testicular cancer, but detection by self-examination is eased with orchiopexy [6]. Clinical presentations of malignant intraabdominal testis can range from an asymptomatic mass to symptoms simulating retroperitoneal mass, incarcerated hernia, urinary frequency or dysuria from mass effect on bladder or acute abdominal pain due to torsion and hemorrhage [7]. In our case, the left testis was intra-abdominal, the patient did never seek medical advice before, about his hemiscrotal emptiness. Our decision was an urgent exploration after a detailed physical examination of the abdomen and genitalia, meticulous inspection of radiological films and, above all, the awareness of rupture and instability.
An acute abdomen with a notion of cryptorchidism should make us think more often of a torsion of an intraabdominal testicular tumor, even if it is a rare diagnosis.
The authors declare no competing interests.
Houssame Lachhab wrote the article, Adil Kbirou helped take pictures, Yassine Harmoumi did the radiological exams, the other authors contributed to the therapeutic management of the disease and to the writing of this document. All authors have read and approved the final version of this manuscript.
Figure 1: showing mass (arrow)
Figure 2: intra-operative view
Figure 3: intra-operative view
Figure 4: histopathology showing seminoma
- Rathmell WK, Godley PA. 86 - Cancer du testicule. In: Runge MS, Greganti MA, éditeurs Médecine interne de Netter Paris : Elsevier Masson. 2011;671-9.
- Hussain S. Torsion of a giant intra-abdominal testicular seminoma presenting as acute abdomen. Indian J Surg. 2015 Apr;77(Suppl 1):64-5. PubMed | Google Scholar
- Sapin E. Ectopie testiculaire et cryptorchidie; de quoi parle-t-on? Indications opératoires. Arch Pédiatrie. 2014 Jan;21(1):113-7. PubMed | Google Scholar
- Zilberman D, Inbar Y, Heyman Z, Shinhar D, Bilik R, Avigad I et al. Torsion of the cryptorchid testis-can It be salvaged. J Urol. 2006;175(6):2287-9. PubMed | Google Scholar
- Ghobashy A, Hasan D, AbdElsalam A, Ahmed A, Arafat A, Tarek M et al. Acute abdomen caused by rupture of a torted intra-abdominal testicular mass: case report. Int J Surg Case Rep. 2020;68:224-7. PubMed | Google Scholar
- Naouar S, Braiek S, El Kamel R. Testicular torsion in undescended testis: a persistent challenge. Asian J Urol. 2017;4(2):111-5. PubMed | Google Scholar
- Mohapatra M, Satyanarayana S, Mishra A, Rao KVR, Rao GB. Seminoma of undescended testis presenting as acute abdomen. Indian J Pathol Microbiol. 2009;52(2):278. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures


Article metrics

