
Wellens´ syndrome: about two cases
Mehdi Ben Lassoued, Sami Kouki, Manel Kallel, Rania Jebri, Houaida Mahfoudhi, Khaled Lamine
Corresponding author: Mehdi Ben lassoued, Emergency Department, Military Hospital of Tunis, Tunis, Tunisia 
Received: 19 Jul 2020 - Accepted: 24 Jul 2020 - Published: 03 Feb 2021
Domain: Cardiology
Keywords: Wellens’ syndrome, electrocardiographic changes, emergency, myocardial infarction
©Mehdi Ben Lassoued et al. PAMJ Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Mehdi Ben Lassoued et al. Wellens´ syndrome: about two cases. PAMJ Clinical Medicine. 2021;5:51. [doi: 10.11604/pamj-cm.2021.5.51.25074]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com//content/article/5/51/full
Case report 

Wellens´ syndrome: about two cases
Wellens´ syndrome: about two cases
Mehdi Ben Lassoued1,&, Sami Kouki2, Manel Kallel1, Rania Jebri1, Houaida Mahfoudhi3, Khaled Lamine1
&Corresponding author
Wellens´ syndrome is a pattern of electrocardiography T-wave changes associated with critical proximal left anterior descending artery lesion. Patients with Wellens' syndrome are at high risk of the development of extensive myocardial infarction of the anterior wall and death. Thus, it becomes crucial that emergency department physicians recognize these patients promptly. We report in this article, two cases of Wellens' syndrome to study its epidemiological, clinical, electrical and therapeutic characteristics.

Wellens' syndrome was first described in 1982 by HJ Wellens. «It was characterised by episodes of unstable angor associated with an inverted T-wave in the anterior derivations». This presentation is associated with a higher risk of anterior myocardial infarction (MI) and/or sudden death related to a critical stenosis of the proximal left anterior descending (LAD) artery lesion.

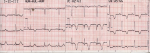
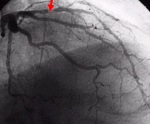
Case N°1: this case is about a 44-year-old female smoker at 10 packs/year, with no medical history. She presented to the emergency department with a crushing chest pain of one month standing which radiated to the back. The pain occurred in attacks of a few minutes at rest. The attacks were getting more and more frequent and increasingly painful. The patient also complained of increasingly severe dyspnea on exertion. On physical examination, the patient was afebrile; her BP 100/50 mmHg in both arms, her heartbeat at 82 bpm, her respiratory frequency at 16 cpm and her SpO2 at 100% on room air. There were no signs of acute heart failure. Electrocardiography (ECG) showed antero-septo-apical negative T-waves (Figure 1). The diagnosis of Wellens´ syndrome was made. The patient was given a dual anti-platelet (aspirin and clopidogrel) and anti-thrombosis (subcutaneous low molecular-weight heparin) treatment. She was referred to the cardiology department where a coronary angiography revealed double-vessel-coronary lesions, a subocclusive stenosis of the medium anterior interventricular artery and an important short stenosis of the ostium of the second marginal branch involving the origin of a collateral branch (Figure 2). Primary percutaneous transluminal coronary angioplasty (PTCA) of the medium anterior interventricular artery was performed consisting in implantation of a radioactive stent without prior dilatation.
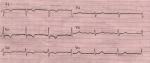
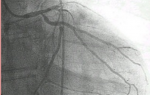
Case N°2: this case is about a 73-year-old hypertensive woman (whose hypertension was newly diagnosed), who had been complaining for 2 months of chest pain and exertional dyspnea. She was referred to our emergency department by a cardiologist in private practice for electrocardiographic abnormalities of recent onset. On admission, the patient was not in pain, her BP 140/80mmg Hg, heartbeat at 75 bpm with no signs of acute heart failure. Her ECG revealed an antero-septal sub-epicardial ischemia (Figure 3). Cardiac laboratory tests were negative. Coronary angiography performed at hour 12 showed an occluded anterior interventricular artery in its proximal portion with a tight ostial circumflex (Figure 4). Management consisted in a double by-pass of Intraoperative Vascular Angiography (IVA) and of the circumflex. Echography did not show any segmentary kinetic disorders. The obtained ventricular ejection fraction (LVEF) was estimated at 50%. The patient was discharged free of complications.
Initially described by Gerson et al. in 1980 then by Wellens in 1982, this syndrome is defined by the inversion of the T-waves. It is the expression of a severe stenosis of the proximal LAD leading in 75% of cases to anterior myocardial infarction within a few days [1]. The pathophysiology of Wellens´ syndrome ECG manifestations in relation to proximal LAD lesions is not fully understood, and it has been suggested that development of T-wave inversion with resolution of symptoms represents a phase of reperfusion [2]. In Wellens´ first study, in 26 out of 145 patients admitted for unstable angina (8%), ECGs showed changes which developed during the pain-free period [1]. In the later prospective study, 180 out of 1,260 hospitalized patients (14%) showed the characteristic electrocardiographic changes [3]. Urgent coronary angiography was implemented, and all of the 180 patients with electrocardiographic changes were found to have blockage of the LAD, varying from 50% to complete obstruction [3]. Diagnosis is established by the evidence of inverted T-waves on ECG performed in the intercritical period. The characteristic electrocardiographic pattern often develops when the patient is not experiencing angina. This electrical sign is the expression of the resumption of the myocardial perfusion. ECG changes in V2-V3 only, reveal a lesion in the segments 1 and 2 of the septal branch of LAD. However, when the lesion is more proximal, the changes involve the precordial derivations. Diagnostic clues of Wellens' syndrome are given in Table 1. There are two types (A and B) of ECG changes occurring in Wellens' syndrome (Figure 5): biphasic T waves in leads V2 et V3 (type I) and deeply inverted T waves in leads V2 and V3 (type II), both suggesting substantial “preinfarction” lesions.
Type A occurs in 75% to 80% cases of Wellens´ syndrome; the remaining 20% to 25% represents type B and shows much more subtle findings of smaller biphasic T-waves across the anterior leads, most commonly leads V2 to V3 and occasionally leads V1 and V4 to V6 [4]. While the differential diagnosis for T-wave inversions is broad, abnormalities found in Wellens´ syndrome are particularly of concern because they often occur in asymptomatic patients, they might pseudonormalize in those presenting with cardiac chest pain or dyspnea, and they will not typically elevate cardiac enzymes. The concern is that ECGs might be interpreted as “nonspecific ST-segment or T-wave changes” in patients with identified risk factors for coronary artery disease who are then sent for outpatient Stress Test [5]. Numerous cases in the literature describe patients with these ECG abnormalities sent for stress test who experience fatal myocardial Infarction during testing [4,6,7]. In fact, performing exercise stress tests for these patients can be fatal due to severe stenosis that might lead to infarction at the time of increased cardiac demand [8]. As cardiac enzyme test results are often negative or within the upper limit of normal, ECG interpretation might be the only clue to the safest disposition of these patients. These ECG abnormalities can be found in a range of patients, including those as young as 39 years of age [9] and those with previously stented LAD lesions or recurrent Wellens´ syndrome [10]. Emergency physicians should be able to recognize these ECG changes and must be aware of their importance so that they can prescribe the correct treatment.
Wellens' syndrome is a clinico-electrocardiographic entity which reveals precise anatomic lesions in AIV in its proximal portion that must be recognized by the emergency physician. Accurate identification of patients with Wellens´ syndrome allows more rapid and appropriately aggressive management. It becomes crucial that emergency department physicians recognize these patients to prevent prolonged staying in emergency department and inappropriate conservative therapy.
The authors declare no competing interests.
All the authors have read and agreed to the final manuscript.
Table 1: criteria for diagnosis of Wellens´ syndrome
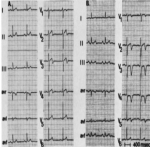
Figure 1: deeply inverted T-waves in antero-septo-apical leads
Figure 2: image of the coronarography showing coronary stenosis
Figure 3: electrocardiography showing antero-septal sub-epicardial ischemia
Figure 4: image of the coronarographie showed an occluded anterior interventricular artery in its proximal portion with a tight ostial circumflex
Figure 5: types of Wellens´ syndrome
- Zwaan Chris, Frits Bär, Wellens Hein. Characteristic electrocardiographic pattern indicating a critical stenosis high in the left anterior descending coronary artery in patients admitted because of impending myocardial infarction. Am Heart J. 1982;103(4):730-736. PubMed | Google Scholar
- Federico Migliore, Alessandro Zorzi, Martina Perazzolo, Cristina Basso, Francesco Corbetti, Manuel De Lazzari et al. Myocardial edema underlies dynamic T-wave inversion (Wellens´ ECG pattern) in patients with reversible left ventricular dysfunction. Heart Rhythm. 2011;8(10):1629-1634. PubMed | Google Scholar
- Zwann Chris, Bar Frits. Angiographic and clinical characteristics of patients with unstable angina showing an ECG pattern indicating critical narrowing of the proximal LAD coronary artery. Am Heart J. 1989;117(3):657-665. PubMed | Google Scholar
- Rhinehardt Joseph, Brady William, Perron Andrew, Mattu A. Electrocardiographic manifestations of Wellens´ syndrome. Am J Emerg Med. 2002;20(7):638-643. PubMed | Google Scholar
- Parikh Kishan, Agarwal Rajiv, Mehrota Amit, Swamy Rajiv. Wellens syndrome: a life-saving diagnosis. Am J Emerg Med. 2012;30(1):253-255. PubMed | Google Scholar
- Lilaonitkul Maytinee, Robinson Ken, Roberts Mark. Wellens´ syndrome: significance of ECG pat- tern recognition in the emergency department. Emerg Med J. 2009;26(10):750-751. PubMed | Google Scholar
- Tandy Tamdy, Bottomy David, Lewis Joseph. Wellens´ syndrome. Ann Emerg Med. 1999;33(3):347-351. PubMed | Google Scholar
- Ersan Tatli, Meryem Aktoz. Wellens´ syndrome: the electrocardiographic finding that is seen as unimportant. Cardiol J. 2009;16(1):73-75. PubMed | Google Scholar
- Corrao Salvatore, Amico Salvatore, Calvo Luigi, Barone Eliana, Licata Giuseppe. An uncommon clinical picture: Wellens´ syndrome in a morbidly obese young man. Intern Emerg Med. 2010; 5(5):443-445. PubMed | Google Scholar
- Nisbet Bruce, Zlupko George. Repeat Wellens´ syndrome: case report of critical proximal left anterior descending artery restenosis. J Emerg Med. 2010;39(3):305-308. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures
Article metrics
PlumX Metrics
Wellens´ syndrome: about two cases
