
Wolf-Parkinson-White syndrome
Najlaa Salmi, Zouhair Lakhal
Corresponding author: Najlaa Salmi, Department of Cardiology, Mohammed V Military Hospital, Mohammed V University, Rabat, Morocco 
Received: 22 Dec 2020 - Accepted: 03 Apr 2021 - Published: 06 Apr 2021
Domain: Cardiology
Keywords: Electrocardiogram, Wolff-Parkinson-White, palpitations
©Najlaa Salmi et al. PAMJ Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Najlaa Salmi et al. Wolf-Parkinson-White syndrome. PAMJ Clinical Medicine. 2021;5:82. [doi: 10.11604/pamj-cm.2021.5.82.27533]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com//content/article/5/82/full
Images in clinical medicine 

Wolf-Parkinson-White syndrome
Wolf-Parkinson-White syndrome
![]() Najlaa Salmi1,&, Zouhair Lakhal1
Najlaa Salmi1,&, Zouhair Lakhal1
&Corresponding author

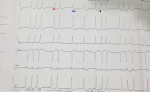
We report the case of a 59-year-old patient with no cardiovascular risk factors and medical history. He consults in the emergency room for rapid onset of palpitations with precordial pain. Clinical examination was normal. The electrocardiogram shows a short PR interval <120 ms, an initial QRS foot base, enlargement of the QRS complexes with repolarization anomalies. Wolf Parkinson White syndrome is defined by the presence of a permeable accessory pathway (Kent bundle) leading to ventricular pre-excitation which by passes the normal conduction. The ventricular myocardium is therefore depolarized in advance by the accessory bundle, which results in a fusion between the first atrioventricular activation and that the one that passes through the normal pathway. The electric aspect combines a short PR interval <120 ms, an initial QRS foot base called the delta wave, an enlargement of the QRS complex with frequent repolarization anomalies. The pre-excitation of wolf parkinson white is usually asymptomatic. Tachycardia and/or arrhythmia may cause the following symptoms: palpitations, dizziness, faintness, syncope, chest pain, and sudden death. It had numerous etiologies: idiopathic, Epstein's disease, coronary artery disease, hyperthyroidism, or high blood pressure. Episodes of paroxysmal supraventricular tachycardia due to Wolff Parkinson's white syndrome can be stopped by any vagal maneuver which slows the heart rate. When these maneuvers are ineffective, drugs such as verapamil and adenosine are usually used to stop the arrhythmia. Arrhythmic drugs can then be taken indefinitely to prevent further episodes. Catheter ablation of the accessory bundle is successful in over 95% of cases.
Figure 1: the electrocardiogram shows a short PR interval <120 ms (red arrow), an initial QRS foot base (black arrow), enlargement of the QRS complexes with repolarization anomalies (blue arrow)
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Article metrics
PlumX Metrics
Wolf-Parkinson-White syndrome
