
Early death from COPD related to occupational exposure to gypsum dust: a case report
Nehla Rmadi, Feriel Dhouib, Nada Kotti, Imen Sellami, Kaouthar Jmal Hammami, Mohamed Larbi Masmoudi, Mounira Hajjaji
Corresponding author: Nehla Rmadi, Department of Occupational Medicine, Hospital Hedi Chaker, Sfax, Tunisia 
Received: 01 Sep 2021 - Accepted: 27 Jan 2022 - Published: 27 Jan 2022
Domain: Biostatistics,Work environment
Keywords: Chronic obstructive pulmonary disease, occupational exposure, dust, case report
©Nehla Rmadi et al. PAMJ Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Nehla Rmadi et al. Early death from COPD related to occupational exposure to gypsum dust: a case report. PAMJ Clinical Medicine. 2022;8:20. [doi: 10.11604/pamj-cm.2022.8.20.31469]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com//content/article/8/20/full
Case report 

Early death from COPD related to occupational exposure to gypsum dust: a case report
Early death from COPD related to occupational exposure to gypsum dust: a case report
![]() Nehla Rmadi1,&,
Nehla Rmadi1,&, ![]() Feriel Dhouib1,
Feriel Dhouib1, ![]() Nada Kotti1,
Nada Kotti1, ![]() Imen Sellami1,
Imen Sellami1, ![]() Kaouthar Jmal Hammami1,
Kaouthar Jmal Hammami1, ![]() Mohamed Larbi Masmoudi1,
Mohamed Larbi Masmoudi1, ![]() Mounira Hajjaji1
Mounira Hajjaji1
&Corresponding author
Chronic obstructive pulmonary disease (COPD) is considered as a fatal but a preventable disease. It occurs rather in the elderly and often after smoking intoxication over many years. However, it may strike younger people particularly, due to a complex interaction between genes and the environment. We report a case of a 34-year-old man, a former smoker with a history of occupational exposure to gypsum dust, who has been diagnosed with end-stage COPD. Tobacco smoke and occupational exposure to gypsum dust were thought to interact in the development and the progression of this early COPD. Thus, physicians must be aware of the potential occupational aetiologies for COPD and should consider them in patients particularly when it occurs at an early age.

Nowadays, chronic obstructive pulmonary disease (COPD) is the third leading cause of death worldwide [1]. Tobacco smoking is the main leading cause of COPD in more than 90% of the cases [2]. It has always been considered a disease of the elderly, since it is generally diagnosed over the age of 45, after several years of smoking [3]. Although it is not new, little attention has been paid to the concept of early COPD from a pathophysiological point of view. It is generally related to genetic factors, mainly the alpha-1 antitrypsin deficiency [4]. However, it can also be caused through environmental exposure such as occupational factors especially when associated to a smoking history [5]. We report the case of a man that developed a stage 4 COPD at very young age (34 years) due to synergetic effects between smoking and occupational exposure to gypsum dust. This condition led him to the death, 4 years from disease´s diagnosis.

Patient information: a 34-year-old man, ex-smoker for 25 pack-years weaned at the age of 33 presented to the department of pneumology with acute dyspnea and symptomatology of hypercapnic encephalopathy requiring non-invasive ventilation.
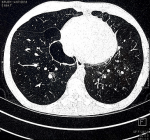
Clinical findings and diagnostic assessment: a chest X-ray revealed an evidence of hyperexpansion and bullous emphysema predominantly affecting the upper zones (Figure 1). A constrictive COPD with paraseptal emphysema and pulmonary hypertension were shown in the pulmonary computed tomogram (Figure 2). Once stabilized, on the 21st day after admission, the patient underwent spirometry with bronchodilator test which indicated a persistent airflow obstruction pattern and a very severe COPD (stage 4) (Table 1). Post-bronchodilator spirometry showed partially reversible airflow obstruction with an increase in FEV1 of only 6%, much less than the reversible airflow obstruction seen in bronchial asthma.
Therapeutic interventions: the patient was treated with oxygen therapy, nebulisation with salbutamol, budesonide and ipratropium bromide, and was given supportive therapy including intravenous fluids, antibiotics and mucokinetics.
Follow-up and outcomes: face to this case of early COPD, it was reasonable to consider other risk factors besides to smoking. Therefore, alpha 1 antitrypsin level was normal. In addition to this medical history, patient´s occupational history was taken in order to identify any association between occupational exposure and the onset of COPD at that early age. In fact, he worked as a plasterer and had 9 years of occupational exposure to gypsum dust. There was no personal protective equipment or ventilation in the workplace. His respiratory symptoms have just appeared 6 years since hiring.
Patient perspective: the patient had a rapid worsening of the condition and died only 4 years from disease´s diagnosis, after multiple hospitalizations for acute exacerbations ending by a respiratory failure.
Informed consent: informed consent was obtained from the patient prior to collecting data and issuing iconography.
Early COPD is a heterogeneous and a rare condition. It is defined according to the age and smoking status, by the occurring of COPD before 50 years for ever-smokers (≥10 pack-years) [6]. It is well known that cigarette smoking is the strongest risk factor for COPD and that it interacts with aging for the development of this disease [7]. The present patient was diagnosed with very severe COPD at the age of 32. Although he had been a smoker, the identification of other precipitating factors that may explain this early onset was adequate. In fact, smoking is not the only risk factor, since that many non-smokers have developed this disease [8]. Another main established risk factor for the development of early COPD is deficiency of alpha-1-antitrypsin [9]. Considering this fact, the patient was tested for this enzyme and had normal level. In addition to genetic factors, environmental triggers, such as occupational hazards can be implied in the development of COPD during early adulthood [10]. From a pathophysiological point of view, innate and adaptive immune systems play a major role in early COPD-onset. The resulting immune responses might occur at the same time early in life as a result of individual susceptibility to several factors apart from active cigarette smoking, such as exposure to dust determining the development of airflow obstruction at a young age [11]. In the present case, besides smoking, the patient had worked in the construction industry and had an occupational history of habitual exposure to gypsum dust during 9 years. He had developed respiratory symptoms just 6 years since hiring. Thus, occupational exposure was suspected being responsible for the rapid aggravation of this very severe COPD. In fact, there was a synergistic effect between smoking and occupational exposure to dust on the onset of COPD. Indeed, even after adjustment for smoking history in many studies, dust exposure can amplify on their own the risk of developing COPD among smokers independently of the effects of cigarette smoking [12].
Published research findings suggested that work related exposures to toxic fumes and dusts may be the cause of many cases of COPD [13,14]. The building and construction industry is a major sector in which workers are daily exposed to non-specific construction dust, which increases the risk of COPD [15]. This association was found particularly among plasterers exposed to gypsum dust such as the case of this patient [16]. In addition to that, occupational exposures may not only be associated with COPD, but may carry a risk of more severe disease once established [17]. The present patient died from a very severe COPD at a very young age (36 years). Some authors suggested that occupational exposure among construction workers increases mortality due to COPD, even among never-smokers [18]. Moreover, the absence of proper collective and personal means of protection in the workplace may explain the severity of the COPD in this case. Compared to developed countries, workers in developing countries are exposed to high levels of dust due to lack of adequate protection and lack of strict regulations in the workplace [19]. Personal protective equipment compliance can minimize health hazards, increase productivity, and ultimately life expectancy [20]. These findings suggest that along with smoking from an early age, the inhalation of gypsum dust may induce early-onset of COPD in a patient with a normal alpha-1-antitrypsin level.
COPD is generally related to a complex interaction between tobacco smoking and aging. Occurring at an early age, other precipitating factors for COPD should be suspected especially occupational ones. In the present case, the identification of the occupational aetiology at an early stage with the implementation of proper protection measures would have prevented the rapid fatal evolution of this disease. Thus, an occupational history should be an important step in the COPD diagnostic process.
The authors declare no competing interests.
All authors have read and agreed to the final manuscript.
Table 1: the results of spirometry before and after bronchodilator test
Figure 1: chest radiograph demonstrating hyper inflated lung fields
Figure 2: computed tomogram image indicating paraseptal emphysema peripheral, bilateral paracardiac bullous and pulmonary hypertension
- World Health Organization. The top 10 causes of death. Accessed October 21, 2020.
- Younus M, Choudhry MK, Syed ZA, Mushtaq W. Role of spirometry in the early diagnosis of chronic obstructive pulmonary disease in smokers. Pak J chest Med. 2015;16(2). Google Scholar
- Holm KE, Plaufcan MR, Ford DW, Sandhaus RA, Strand M, Strange C et al. The impact of age on outcomes in chronic obstructive pulmonary disease differs by relationship status. Int J Behav Med. 2014;37(4):654-63. PubMed | Google Scholar
- Ioachimescu OC, Stoller JK. A review of alpha-1 antitrypsin deficiency. COPD. 2005;2(2):263-75. PubMed | Google Scholar
- Alif SM, Dharmage SC, Bowatte G, Karahalios A, Benke G, Dennekamp M et al. Occupational exposure and risk of chronic obstructive pulmonary disease: a systematic review and meta-analysis. Expert Rev Respir Med. 2016;10(8):861-72. PubMed | Google Scholar
- Martinez FJ, Han MK, Allinson JP, Barr RG, Boucher RC, Calverley PM et al. At the root: defining and halting progression of early chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;197(12):1540-51. PubMed | Google Scholar
- Kim EJ, Yoon SJ, Kim YE, Go DS, Jung Y. Effects of aging and smoking duration on cigarette smoke-induced COPD severity. J Korean Med Sci. 2018 Nov 27;34(Suppl 1):e90. PubMed | Google Scholar
- Salvi SS, Barnes PJ. Chronic obstructive pulmonary disease in non-smokers. Lancet. 2009 Aug 29;374(9691):733-43. PubMed | Google Scholar
- Cazzola M, Stolz D, Rogliani P, Matera MG. α1-antitrypsin deficiency and chronic respiratory disorders. Eur Respir Rev. 2020 Feb 12;29(155):190073. PubMed | Google Scholar
- Postma DS, Bush A, van den Berge M. Risk factors and early origins of chronic obstructive pulmonary disease. Lancet. 2015;385(9971):899-909. PubMed | Google Scholar
- Martinez FD. Early-life origins of chronic obstructive pulmonary disease. N Engl J Med. 2016;375(9):871-8. PubMed | Google Scholar
- Boschetto P, Quintavalle S, Miotto D, Cascio NL, Zeni E, Mapp CE. Chronic obstructive pulmonary disease (COPD) and occupational exposures. J Occup Med Toxicol. 2006 Jun 7;1:11. PubMed | Google Scholar
- Guo C, Zhang Z, Lau AKH, Lin CQ, Chuang YC, Chan J α. Effect of long-term exposure to fine particulate matter on lung function decline and risk of chronic obstructive pulmonary disease in Taiwan: a longitudinal, cohort study. Lancet Planet Health. 2018;2(3):e114-e25. PubMed | Google Scholar
- Sana A, Somda SMA, Meda N, Bouland C. Chronic obstructive pulmonary disease associated with biomass fuel use in women: a systematic review and meta-analysis. BMJ Open Respir Res. 2018;5(1):e000246. PubMed | Google Scholar
- Borup H, Kirkeskov L, Hanskov DJA, Brauer C. Systematic review: chronic obstructive pulmonary disease and construction workers. Occup Med (Lond). 2017;67(3):199-204. PubMed | Google Scholar
- Dement JM, Welch L, Ringen K, Bingham E, Quinn P. Airways obstruction among older construction and trade workers at Department of Energy nuclear sites. Am J Ind Med. 2010;53(3):224-40. PubMed | Google Scholar
- Blanc P, Menezes A, Plana E, Mannino D, Hallal P, Toren K et al. Occupational exposures and COPD: an ecological analysis of international data. Eur Respir J. 2009;33(2):298-304. PubMed | Google Scholar
- Bergdahl I, Toren K, Eriksson K, Hedlund U, Nilsson T, Flodin R et al. Increased mortality in COPD among construction workers exposed to inorganic dust. Eur Respir J. 2004;23(3):402-6. PubMed | Google Scholar
- Salvi S. Tobacco smoking and environmental risk factors for chronic obstructive pulmonary disease. Clin Chest Med. 2014;35(1):17-27. PubMed | Google Scholar
- Hamzah NA, Mohd Tamrin SB, Ismail NH. Metal dust exposure and lung function deterioration among steel workers: an exposure-response relationship. Int J Occup Environ Health. 2016;22(3):224-32. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures

Article metrics

