
Swallowed nail perforating the anterior surface of the stomach and penetrating the abdominal wall from the inside: a case report
Ahmed Taha
Corresponding author: Ahmed Taha, Yalova State Hospital, Department of General Surgery, Yalova, Turkey 
Received: 22 Apr 2022 - Accepted: 09 Jun 2022 - Published: 13 Jun 2022
Domain: General surgery
Keywords: Stomach, foreign body, mental retardation, perforation, case report
©Ahmed Taha et al. PAMJ Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Ahmed Taha et al. Swallowed nail perforating the anterior surface of the stomach and penetrating the abdominal wall from the inside: a case report. PAMJ Clinical Medicine. 2022;9:11. [doi: 10.11604/pamj-cm.2022.9.11.35073]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com//content/article/9/11/full
Case report 
Swallowed nail perforating the anterior surface of the stomach and penetrating the abdominal wall from the inside: a case report
Swallowed nail perforating the anterior surface of the stomach and penetrating the abdominal wall from the inside: a case report
![]() Ahmed Taha1,&
Ahmed Taha1,&
&Corresponding author
Foreign body ingestion is a problem generally found in children, some psychological diseases, and people with mental retardation. In most cases, they pass through the gastrointestinal tract, come out with faeces and rarely cause infection, local reaction, migration, or perforation. A computed tomography (CT) scan is the ideal choice for complicated case diagnosis. We report a case of a pointed rusty nail, perforating the stomach from inside, passing through the skin of the abdomen, outward from the left upper quadrant, and successfully extracted by open surgery in a patient with mental retardation. We recommend that we can care for those with mental retardation or who have foreign body ingestion habits by checking them regularly.

Swallowing foreign bodies is a problem generally found in children, some psychological diseases, and people with mental retardation. In the majority of cases, foreign bodies are small and come out with faeces without damaging the gastrointestinal tract. Sometimes endoscopic (10-20%) or surgical interventions (1%) are used [1-3]. Patients or their relatives often apply to health institutions before symptoms begin at the time of the incident. In random cases, swallowed objects are held silent. When they cause infection, local reaction, migration, or perforation, patients apply to the emergency department with abdominal pain, nausea, vomiting, fever, or acute abdomen. Foreign bodies are detected in radiological examinations and surgical procedures are often applied [4-6].

Patient information: a 31-year-old mentally retarded male patient was admitted to the hospital with complaints of a foreign body presenting from the abdomen, abdominal pain, nausea, and fatigue. The patient came standing up and there were no acute abdomen findings. No known history of additional disease or surgery event other than mental retardation.
Clinical findings: a pointed rusty nail passing through the skin of the abdomen outward from the upper left quadrant was seen. Abscess material is actively flowing around the nail. There was a painful swelling on the abdominal wall in anamnesis that lasted for nearly one month. It was perforated in the last few hours and the nail appeared (Figure 1).
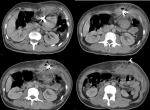
Diagnostic assessment: in the examinations, blood pressure was found to be 105/60 mmHg, fever at 36.6°C, WBC at 21.95 103/mm3, HGB at 11.2 g/dl, PLT at 578 103/mm3 and CRP at 153.3 mg/L were found. A nail was seen in the standing direct abdominal X-ray (Figure 2). The FAST ultrasound reported 8x4 cm of a loculated fluid collection in the upper left quadrant of the anterior abdomen with a dense septum and air echogenicity, and the intra-abdominal relationship could not be evaluated. The CT scan reported a metallic structure extending from the stomach region to the outside of the skin on the left side of the epigastrium (Figure 3).
Diagnosis: diagnosis of foreign body perforation was made.
Therapeutic interventions: after taking the necessary family consent, preparations phases were made, and the patient was taken to the operation immediately. The abdomen was entered with an upper median umbilical incision. A 25 cm nail perforating the anterior surface of the stomach, peritoneum, skin, and subcutaneous layers was extracted (Figure 4). The inside of the stomach was checked, there were no other foreign bodies. There was an abscess cavity under the skin. The stomach was repaired by wedge resection. The abscess was drained. Subcutaneous and peritoneal necrotic areas were debrided. E. coli was grown in the abscess culture. Appropriate antibiotics were given.
Follow-up and outcome of interventions: the patient was discharged seven days after the operation with a PPI drug. No complications developed in the early follow-up. In the 6th month, a gastrostomy was performed, and no significant problem was observed.
Patient perspective: although our communication with the patient was limited, his happiness and satisfaction were quite evident. During the postoperative period, the patient's restraint was evident from his constant smile in the ward, not attempting to pull cannulas, dressings or drains.
Informed consent: all necessary consent documents to publish images and clinical information relating to the case were obtained from the patient's relatives and written in Turkish.
Swallowed foreign bodies are usually small, do not disrupt body integrity, and do not penetrate the body outward. Cases of large and pointed foreign bodies are extremely rare. Complicated cases cause internal perforation or the same reactions. A case of a swallowed foreign body perforating the abdomen from the inside has not been reported in the literature. Interestingly, a long pointed foreign body which has been swallowed before was leaning on the back of the stomach and its pointed part was perforating the front. Foreign body ingestion is usually seen in children, alcoholics, and those with mental retardation. In 80% of the cases, they pass the GIS without causing serious problems. Endoscopic procedures can be applied in noticed cases [7,8]. Cases of complicated foreign bodies are often detected in radiological examinations of patients with chronic complaints. Metallic and hard objects are seen on standing radiographs. Even if the reactions caused by the foreign body are seen on the ultrasound, it is difficult to detect them [1-5]. A CT scan is the ideal choice for detecting foreign bodies, visualizing inflammation, and changes in the environment [9].
In this case, we thought that people with mental retardation don´t receive the care or attention they may need, that pointed foreign bodies, such as in our case, could have caused more mortal consequences. For this reason, it is recommended that those who cannot express themselves, those with mental retardation, and especially those who have foreign body ingestion habits, should be checked regularly, and if there are repeated abdominal pain complaints, they should be examined in detail. We may need to inform the public about this.
The author declares no competing interests.
The author have read and agreed to the final manuscript.
Figure 1: a pointed rusty nail passes through the skin of the abdomen outward from the upper left quadrant
Figure 2: the nail was seen in the standing direct abdominal X-ray
Figure 3: the CT scan series
Figure 4: extracting the nail by open surgery
- Webb WA. Management of foreign bodies of the upper gastrointestinal tract: update. Gastrointest Endosc. 1995 Jan;41(1):39-51. PubMed | Google Scholar
- Bolton SM, Saker M, Bass LM. Button battery and magnet ingestions in the pediatric patient. Curr Opin Pediatr. 2018 Oct;30(5):653-659. PubMed | Google Scholar
- Fernando AR, Bulathsinghela R, Samarasekera DN. An unusual cause of small bowel obstruction due to an ingested mango seed: a case report. BMC Res Notes. 2017 Nov 2;10(1):549. PubMed | Google Scholar
- Ambe P, Weber SA, Schauer M, Knoefel WT. Swallowed foreign bodies in adults. Dtsch Arztebl Int. 2012 Dec;109(50):869-75. PubMed | Google Scholar
- Khorana J, Tantivit Y, Phiuphong C, Pattapong S, Siripan S. Foreign body ingestion in pediatrics: distribution, management, and complications. Medicine (Kaunas). 2019 Oct 14;55(10):686. PubMed | Google Scholar
- Smith MT, Wong RK. Foreign bodies. Gastrointest Endosc Clin N Am. 2007 Apr;17(2):361-82. PubMed | Google Scholar
- Kramer RE, Lerner DG, Lin T, Manfredi M, Shah M, Stephen TC et al. Management of ingested foreign bodies in children: a clinical report of the NASPGHAN Endoscopy Committee. J Pediatr Gastroenterol Nutr. 2015 Apr;60(4):562-74. PubMed | Google Scholar
- Bezabih YS, Wonde TE, Ebrahim SH. Perforation of the cecum from an ingested foreign body in a 14-year-old adolescent with autism spectrum disorder and epilepsy: a case report. Int J Surg Case Rep. 2021 Nov;88:106580. PubMed | Google Scholar
- Birk M, Bauerfeind P, Deprez PH, Häfner M, Hartmann D, Hassan C et al. Removal of foreign bodies in the upper gastrointestinal tract in adults: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy. 2016 May;48(5):489-96. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures



Article metrics

