
Body mass index trends and overweight/obesity risk among patients initiating antiretroviral therapy in Bobo-Dioulasso Day Hospital, Burkina Faso: a cohort study from 2002 to 2019
Arsène Hema, Armel Poda, Jacques Zoungrana, Jean Baptiste Tougouma, Clément Meda, Euloges Kamoulé, Abdoul Salam Ouedraogo, Adrien Bruno Sawadogo, Athanase Millogo, Léon Savadogo
Corresponding author: Arsène Hema, Day Hospital, Infectious Diseases, Department of Sourô Sanou University Hospital, Bobo-Dioulasso, Burkina Faso 
Received: 05 May 2022 - Accepted: 03 Aug 2022 - Published: 04 Aug 2022
Domain: HIV epidemiology
Keywords: HIV, antiretroviral therapy, body mass index, overweight/obesity
©Arsène Hema et al. PAMJ Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Arsène Hema et al. Body mass index trends and overweight/obesity risk among patients initiating antiretroviral therapy in Bobo-Dioulasso Day Hospital, Burkina Faso: a cohort study from 2002 to 2019. PAMJ Clinical Medicine. 2022;9:28. [doi: 10.11604/pamj-cm.2022.9.28.35317]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com//content/article/9/28/full
Research 
Body mass index trends and overweight/obesity risk among patients initiating antiretroviral therapy in Bobo-Dioulasso Day Hospital, Burkina Faso: a cohort study from 2002 to 2019
Body mass index trends and overweight/obesity risk among patients initiating antiretroviral therapy in Bobo-Dioulasso Day Hospital, Burkina Faso: a cohort study from 2002 to 2019
![]() Arsène Hema1,&, Armel Poda1,2,
Arsène Hema1,&, Armel Poda1,2, ![]() Jacques Zoungrana1,2, Jean Baptiste Tougouma2,3,
Jacques Zoungrana1,2, Jean Baptiste Tougouma2,3, ![]() Clément Meda2, Euloges Kamoulé4, Abdoul Salam Ouedraogo1,2, Adrien Bruno Sawadogo1, Athanase Millogo5,
Clément Meda2, Euloges Kamoulé4, Abdoul Salam Ouedraogo1,2, Adrien Bruno Sawadogo1, Athanase Millogo5, ![]() Léon Savadogo2
Léon Savadogo2
&Corresponding author
Introduction: studies have shown a high prevalence of overweight/obesity among people living with HIV (PLHIV) using Antiretroviral Therapy (ART). This study aims to analyze the risks and the trends of overweight/obesity among PLHIV under ART.
Methods: we described trends in BMI in PLHIV on ART in the Bobo-Dioulasso using the day hospital cohort between 2002 and 2019. The incidence of overweight/obesity, defined by a BMI ≥ 25 kg/m2, has been described. Mixed linear regression was used to analyze factors associated with BMI gain. A cox proportional hazards model was used to analyze predictors of the occurrence of overweight/obesity.
Results: a total of 6218 patients, including 4359 women (70.1%), were included in our study. The mean age of patients was 41.1 years ± 10.4, and 52.4% were unemployed. The mean CD4 nadir was 206 cells//μl ± 165. Moreover, 56.1% of patients had CD4 nadir ≤200 cells/μl. The mean BMI was 20.8 kg/m2 ± 3.8, and only 13.8% of patients had a BMI of ≥25kg/m2 at their first visit. Also, 1623 new cases of overweight/obesity were noted during the study, with an incidence of 5.5 per 100 person-years. Factors associated with BMI gain were a long period of ART use, merchant occupation or unemployment, HIV diagnosis following clinical suspicion, clinical severity, and CD4 nadir ≤400 cells/μl. The predictorsof overweight/obesity occurrence were: age <40 years (aHR = 1.36; CI = 1.18 - 1.57), female (aHR = 1.70; CI = 1.46 - 1.99), merchant occupation (aHR = 1.28; CI = 1.04 -1.57) and salaried employees (aHR = 1.32; CI: 1.09 - 1.59), HIV diagnosis following clinical suspicion (aHR =1.15; CI = 1.03 - 1.27) and baseline CD4 nadir ≤200 cells/μl (aHR = 1.26; CI = 1.03 - 1.55).
Conclusion: in addition to traditional risk factors for overweight/obesity, late initiation of ART is an independent predictor of overweight/obesity among PLHIV.

Overweight and obesity are emerging public health problems. Indeed, according to the World Health Organization (WHO), 39% of adults aged 18 and over were overweight in 2016, and 13% were obese [1]. Being overweight is associated with the development of comorbidities, such as high blood pressure, diabetes, heart disease, and cancers in the general population, responsible for thousands of deaths each year [2,3]. Antiretroviral therapy has drastically reduced HIV-related morbidity and mortality. However, many studies have shown a high prevalence of overweight or related comorbidities in PLHIV on treatment, such as those observed in the general population [4-8]. Comorbidities such as diabetes, coronary heart disease, high blood pressure, and cancers are well described in the HIV-infected population [9-11]. Several factors, including immune activation, chronic inflammation due to HIV, and ART, are at the origin of these pathologies [12,13].
Sub-Saharan Africa is the region of the world most affected by HIV infection. Since the introduction of ART in this region of the world, the eligibility, and criteria to access ART have been gradually relaxed, giving most PLHIV access to the treatment. Thus, eligibility conditions for ART have increased from CD4≤200/μl in 2006 [14] to CD4≤350/μl [15], and since 2016, the WHO has recommended the implementation of the test and treat approach [16]. The latter makes it possible to put patients on treatment regardless of their CD4 level. Some studies have proven the test and treat approach's effectiveness in reducing HIV-related morbidity-mortality and HIV transmission [17-19]. Nevertheless, more research is needed to assess the magnitude and understanding of the determinants of comorbidities associated with HIV and ART in the African context. The control of HIV-related comorbidities and its treatment, such as obesity, is a guarantee for improving the survival and quality of life of PLHIV. The Bobo-Dioulasso day hospital cohort is one of the largest cohorts in Burkina Faso, with PLHIV, which has been followed since 2002. The purpose of this study is to analyze long-term trends in BMI and to determine the prevalence and predictors of overweight/obesity among PLHIV initiating ART at Bobo-Dioulasso day hospital.

Study design and setting: this was a retrospective cohort study design with a descriptive and analytical component. It was conducted using the clinical database (ESOPE) of Bobo-Dioulasso day hospital PLHIV cohort. This unit of the infectious disease department of the Sourô Sanou university hospital is located in Bobo-Dioulasso, which is the second city of Burkina Faso. There, is one of the largest cohorts of PLHIV in the country [20]. Our analyses focused on data collected from January 2002 to December 2019.
Study population: included in the study were patients aged 18 years or older, enrolled in the day hospital cohort between 2002 and 2019, and who received at least two medical visits on ART at the Bobo-Dioulasso day hospital. Pregnant women were not included in this analysis.
Variables
Outcome: body mass index, the main outcome, was estimated using the formula weight (kg)/(height in meters)2. Body mass index was estimated at each medial follow-up visit. it was categorized into three modalities ≤18; 19-24.9; ˃25 kg/m2 then in two modalities BMI<25 and BMI≥25.
Predictor: age at inclusion was divided into 4 classes according to quartiles: <30; 30 - 39; 40 - 49 and ≥50 years old. Gender: male and female. Profession grouped into 4 categories: farmer/artisan, merchant, salaried employee, unemployed. Type of HIV: HIV1; HIV2 and HIV1+2. Circumstance of HIV discovery: voluntary screening; clinical suspicion. Clinical classification according to 4 WHO clinical stages (stage1, 2,3,4). Nadir CD4 (number/μl): the lowest CD4 count before ART start. It was recoded into three classes: ≤200; 201 - 400; >400/μl. Initial ART: nucleoside reverse transcriptase inhibitor (NRTI); non-nucleoside reverse transcriptase inhibitor (NNRTI); protease inhibitor (PI);
Data collection: data were extracted from the day hospital cohort clinical database (ESOPE®). ESOPE is a clinical database designed by EPICONCEPT for the follow-up of PLHIV. The ESOPE® database of Bobo-Dioulasso day hospital cohort was established in 2006. The ESOPE® database was first informed by data entry operators, thanks to patient data collected between 2002 and 2007 in medical records. Since 2007, physicians have populated this clinical database in real-time during follow-up visits for PLHIV. At the end of 2019, Bobo-Dioulasso day hospital database ESOPE® had 9737 HIV-infected patients (active patients, lost to follow-up, transferred, and deceased). Sociodemographic and clinical data such as date of birth, gender, profession, circumstance of HIV discovery type of HIV, WHO stage, Initial BMI (kg/m2) were collected at the first patient visit. These patients carried out at least two follow-up medical visits per year, during which a clinical examination was carried out, including weight measurement by a SECA 750 Viva® mechanical scale.
Laboratory analysis: depending on patient clinical condition, every 3 or 6 months, a routine biological evaluation of PLHIV including a count of CD4 T lymphocytes was carried out. The CD4 count was measured on venous blood using a Fascount® brand CD4 counter.
Definitions: overweight/obesity were defined by a body mass index (BMI) ≥25 kg/m2.
Statistical analysis: data extracted from the day hospital database were analyzed using STATA version 13. The sociodemographic, biological, and clinical characteristics of PLHIV at the first medical visit were described. The quantitative variables were their mean ± standard deviation. Qualitative variables were described by their proportion (%). The Chi-squared test was used to compare proportions, while the student´s t-test and the analysis of variance (ANOVA) were used to compare the continuous variables of the different groups. The prevalence of overweight/obesity (BMI>25 kg/m2) at the initial medical visit and its incidence during follow-up in patients with BMI<25 kg/m2 at the initial visit were calculated among PLHIV. A curve described the mean gain in BMI according to Nadir CD4 cell count. Kaplan Meier's method was used to describe the incidence of overweight/obesity during the medical follow-up and the log-rank test to compare overweight/obesity incidence curves according to Nadir CD4 cell count. We used a mixed linear regression model (univariable and multivariable) to identify factors associated with BMI change and a Cox proportional hazard model (univariable and multivariable) to identify overweight/obesity occurrence predictors. The following statistical modeling strategy was used for the mixed linear regression and Cox proportional hazard model: univariate analysis was performed to determine the relevant covariates for the multivariate model. Covariates associated with the overweight/obesity occurrence variable at the 20% threshold and the CD4 nadir (main covariate) were selected in the multivariate models. We then proceeded to reduce the covariates in the model thanks to a manual top-down strategy, subtracting at each step the covariate that had the highest significance threshold above 0.05. Nadir CD4 cell count, when not significantly related to overweight/obesity, was forced in all final models. The significance level was 0.05 for all analyzes.
Ethical considerations: in retrospect, it consisted of an analysis of data obtained during routine care that posed no risk to patients. The data extracted from the clinical database (ESOPE) of the Bobo-Dioulasso day hospital have been anonymized to ensure their confidentiality.
Characteristics of patients at the initiation of antiretrovirals (ARV) treatment: of the 9737 patients in the day hospital cohort database, 6218 (63.8%) patients meeting our inclusion criteria were included in this study (Figure 1). The mean Nadir CD4 cell count was 206 cells/μl ± 165. The proportion of patients with Nadir CD4 cell count ≤200 cells/μl, 201-400 cells/μl and >400 cells/μl were respectively 56.1% (n=3487), 33.7% (n=2096), and 10.2% (n=635). Our, 6218 patients were composed of 4359 women (70.1%). The mean age of patients was 41.1 years ± 10.4; the mean Nadir CD4 cell count decreased with age (p=0.000). Our study population was mainly made up of unemployed people (52.4%). Mean nadir CD4 cell counts were statistically different by occupation (p=0.000). Most patients (57.6%, n=3582) had discovered their HIV status following an opportunistic infection, and they accounted for 65.2% of patients with CD4≤200 cell/μl counts. In addition, 44.5% of patients were at stage 3 of the WHO clinical classification of which 63.7% having CD4≤200 cells/μl, (p=0.000). The mean BMI was 20.8 kg/m2 ± 3.8; however, it was estimated at 20.0 kg/m2 ± 3.7 in the group with Nadir CD4 Cell Count ≤200 cells/μl, 21.6 kg/m2 ± 3.8 in the range of Nadir CD4 cell count between 201-400 cells/μl, and 22.2 kg/m2 ± 3.8 in those with Nadir CD4 cell count >400 cells/μl (p=0.000). Only 13.8% (n=857) of patients had a BMI >25 kg/m2 at the initial visit; these patients were better represented in the group with Nadir CD4 Cell Count >400 cells/μl; p=0.000 (Table 1). Patients were mostly (96.8%) on therapeutic combinations made of 2INTI + 1 INNTI.
Evolution: the mean time on ART was 6.2 years ± 4.5. It was 6.1 years ± 4.7 years for patients with CD4≤200 cells/μl, 6.6 years ± 4.2 years for the group of patients with CD4 counts between 201-400 cells/μl and 5.7 years ± 4.6 years in patients with CD4 >400 cells/μl (p=0.000). During follow-up, we observed 512 (8.2%) transfers to other health centers, 667 (10.7%) deaths, and 982 (15.8%) loss to follow-up.
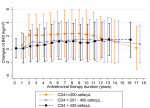
Gain in BMI: the mean gain in BMI was 1.4 kg/m2 ± 3; it was generally higher in patients with Nadir CD4 Cell Count ≤200 cells/μl (1.8 kg/m2 ± 3.2) than in the group with CD4 between 201-400 cells/μl (1.1 kg/m2 ± 2.7), and CD4> 400 CD4/μl (0.6 kg/m2 ± 2.4) p=0.000. The curve of the mean BMI gain of patients with Nadir CD4 cell count ≤200 cells/μl grows faster than those of CD4 between 201 - 400 cells/μl, and CD4 >400 cells/μl; however, it shows a slight inflection from the 11th year to join those of the other two which have a slow and relatively constant evolution (Figure 2).
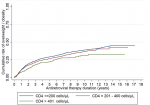
Incidence of overweight/obesity: of the 6218 patients in our study, 857 were overweight or obese at the first medical visit. Among the 5361 patients with a BMI <25 kg/m2 at the first visit, 1623 (30.3%) new cases of overweight/obesity were observed during a total observation period of 2.9 x 104 person-years. The incidence of obesity/overweight was then 5.5 per 100 person-years. It was 5.8 per 100 person-years in patients with a Nadir CD4 cell count ≤200 cells/μl, 5.3 per 100 person-years in those with a Nair CD4 cell count between 201-400 cells/μl and 4.8 per 100 person-years in the CD4>400cell/μl group. The incidence of overweight/obesity increases with the duration of treatment (Figure 3). This incidence was generally different in the three groups (p=0.007).
Factors associated with BMI gain: after multivariable analysis by mixed linear regression, it is observed that the long duration of ART was associated with an increase in BMI. Merchant occupation and unemployment were associated with a mean gain in BMI significantly higher than farmers/artisans and salaried employees. Compared to voluntary testing, HIV diagnosis following clinical suspicion was associated with a higher gain of BMI. The mean gain in BMI increases significantly with the stage of WHO clinical severity. An initial BMI >18 kg/m2 was associated with a significant decrease in BMI. Patients with a CD4≤400 cell/μl nadir had a higher BMI than those with more than 400 CD4/μl. Taking a protease inhibitor-based combination therapy was associated with a decline in BMI (Table 2).
Predictors of overweight/obesity: after multivariable analysis only the age <40 years (aHR=1.36; CI=1.18 - 1.57), female (aHR=1.70; CI=1.46 - 1.99), merchant's occupation (aHR = 1.28; CI = 1.04 - 1.57) and salaried employees (aHR = 1.32; CI: 1.09 - 1.59), HIV diagnosis following clinical suspicion (aHR =1.15; CI = 1.03 - 1.27) as well as Nadir CD4 cell count ≤200 cells/μl (aHR = 1.26; CI = 1.03 - 1.55) were predictive of the occurrence of obesity (Table 3).
Conducted on a PLHIV cohort at Bobo Dioulasso day hospital, the purpose of this study was to analyze BMI trends and determine the incidence and predictors of overweight/obesity in PLHIV initiating ART. From the results of this study, which included 6218 patients, 70.1% of whom were women, we can retain that the mean gain in BMI among PLHIV initiating ART was 1.4 kg/m2 ± 3; it was generally higher in patients with CD4≤200 cells/μl (1.8 kg/m2 ± 3.2). The curve of the mean BMI gain of patients with CD4≤200 cells/μl grows faster to undergo an inflection from the 11th year joining those of CD4 between 201-400 cells/μl and CD4 >400 cells/μl that have slow growth. The prevalence of overweight/obesity was 13.8% at the initial visit, and the incidence of overweight/obesity was 5.5 per 100 person-years. Factors associated with significant BMI gain were long ART duration, merchant's occupation or unemployment, HIV diagnostic following clinical suspicion, clinical severity, and Nadir CD4 cell count ≤400 cell/μl. Predictorsof overweight/obesity were: age <40 years (aHR = 1.36; CI = 1.18 - 1.57), female (aHR = 1.70; CI = 1.46 - 1.99), merchant's occupation (aHR =1.28; CI = 1.04 - 1.57) and salaried employees (aHR =1.32; CI: 1.09 - 1.59), HIV diagnosis following clinical suspicion (aHR = 1.15; CI = 1.03 - 1.27) as well as Nadir CD4 Cell Count ≤200 cells/μl (aHR = 1.26; CI = 1.03 - 1.55).
Before initiating ART, the prevalence of overweight/obesity was 13.8% and lower than the national rate, which was 17.9% [21]. However, in a non-obese population exposed to a mean duration of 6.2 years of ART, we observed a prevalence of overweight/obesity (30.3%) much higher than that of the general population. Bakal et al. [22] observed this same trend in Brazil when comparing the frequency of overweight in PLHIV to the general population. The incidence of overweight/obesity in our study is lower than those of Kintu et al. [23] in Tanzania, Bakal et al. [22] in Brazil, and Koethe et al. [24] in the USA. This fact could be explained by the higher presence of overweight/obesity in their study population at ART initiation. For physiological reasons, women are more susceptible to overweight/obesity than men, as reported by numerous studies in the general population and PLHIV [22-29].
Merchants and salaried employees had an increased risk of overweight/obesity. Most middle and high socioeconomic people are recruited from these groups. Studies in Africa have demonstrated a strong positive relationship between obesity and high socioeconomic status, unlike in developed countries where obesity is instead associated with low socioeconomic status [30,31]. These people tend to consume more convenient and fast ultra-processed foods and access modern technology that promotes a sedentary lifestyle [32]. In antiretroviral-naïve patients, profound immunosuppression is associated with significant weight loss due to recurrent opportunistic infections. Immune restoration is accompanied by more significant weight gain in those with low CD4 patients during the first years of ART. A moderate weight growth phase follows this rapid weight increase phase. This biphasic evolution of the BMI curve in PLHIV initiating ART has been reported in several series [27,33,34]. Low CD4 nadir and the presence of clinical signs of immunosuppression at screening were associated with greater BMI gain and risk factors for overweight/obesity in our study. Our results corroborate those of the literature [22,23,26,28,33,35]. The extreme immune restoration observed after ART initiation in patients with advanced HIV infection may explain relatively high weight gain in these patients [27]. Similarly, the stronger immune response to ART may explain the increased risk of overweight/obesity in young people [22].
Also, some studies suggest the association between overweight/obesity and increased inflammation in highly immunocompromised patients. This inflammation would result in a significant amount of sCD14 in highly immunocompromised patients. It causes dysbiosis associated with overweight/obesity [13,28,36]. Weight gain at ART initiation can be considered a normal and desired phenomenon because it reflects an excellent clinical response to treatment. However, when it is excessive, it puts patients in a state of overweight/obesity and exposes them to a high risk of noncommunicable diseases [37]. The lack of information on behavioral factors such as diet, alcohol consumption, and physical activities of patients is the main limitation of this study. Similarly, the analysis of BMI trends does not concern HIV-positive patients who survive to start ART, which could be a source of survival bias. However, the prospective and longitudinal collection of data in this large observational study is a strong point. Also, the statistical modeling strategy used mixed regression allows control of possible individual heterogeneities to estimate the causal relationships between explanatory variables and the variable of interest [38].
Among PLHIV, overweight and obesity appear to be emerging factors in morbidity and mortality in the era of triple antiretroviral therapy. In addition to traditional risk factors for overweight/obesity, late initiation of ART is an independent predictive factor of overweight/obesity among PLHIV. To prevent obesity and these corollaries among the PLHIV population, they should be encouraged to have a healthy lifestyle: balanced diet, physical activity, alcohol avoidance.
What is known about this topic
- The high prevalence of overweight/obesity among PLHIV on ART;
- HIV, ART and sometimes the CD4 count are mentioned as risk factors for overweight/obesity;
- Overweight/obesity are risk factors for metabolic and cardiovascular pathologies.
What this study adds
- Information on the incidence of overweight/obesity among PLHIV on ART in Burkina Faso;
- The initial CD4 count is a predictor of overweight/obesity;
- Absence of association between ART and overweight/obesity.
The authors declare no competing interests.
Conception and design of study: AH, AP. Acquisition of data: AH, AP, JZ,JBT, EK, ASO. Analysis and interpretation of data: AH, AP, JZ, CM. Guarantor of the study: AM, LS. All the authors have read and agreed to the final manuscript.
All patients followed in Bobo-Dioulasso day hospital, Bobo-Dioulasso day hospital nursing staff.
Table 1: baseline characteristics of 6218 patients followed on ART from 2002 to 2019 at the Bobo-Dioulasso day hospital
Table 2: factors associated with the change of the BMI vs baseline in 6,218 patients followed on ART from 2002-2019 at Bobo - Dioulasso day hospital (mixed linear regression)
Table 3: predictors of overweight/obesity occurrence in 5361 patients with BMI<25 kg/m2 followed under ARV treatment from 2002 -2019 at the Bobo-Dioulasso day hospital
Figure 1: study Inclusion criteria
Figure 2: changes of BMI vs baseline (mean and standard deviation) according to the CD4 nadir cells count category, among 6218 patients followed on ARV treatment from 2002-2019 at the Bobo-Dioulasso day hospital
Figure 3: cumulative risk of overweight / obesity according to the CD4 nadir cells count category among 5361 patients with BMI<25 kg/m2 followed on ARV treatment from 2002-2019 at the Bobo-Dioulasso day hospital
- Food and Agriculture Organization of the United Nations, International Fund for Agricultural Development, United Nations Children´s Fund, World Food Programme, World Health Organization. The state of food security and nutrition in the world 2019; safeguarding against economic slowdowns and downturns. Rome: Food and Agriculture Organization of the United Nations. 2021. Google Scholar
- Chen H, Chen G, Zheng X, Guo Y. Contribution of specific diseases and injuries to changes in health adjusted life expectancy in 187 countries from 1990 to 2013: retrospective observational study. BMJ. 2019 Mar 27;364:l969. PubMed | Google Scholar
- Salomon JA, Wang H, Freeman MK, Vos T, Flaxman AD, Lopez AD et al. Healthy life expectancy for 187 countries, 1990-2010: a systematic analysis for the global burden disease study 2010. The Lancet. 2012 Dec 15;380(9859):2144-62. PubMed | Google Scholar
- Ahmed D, Roy D, Cassol E. Examining relationships between metabolism and persistent inflammation in HIV patients on antiretroviral therapy. Mediators of Inflammation. 2018 Sep 27;2018:6238978. PubMed | Google Scholar
- Chhoun P, Ngin C, Tuot S, Pal K, Steel M, Dionisio J et al. Non-communicable diseases and related risk behaviors among men and women living with HIV in Cambodia: findings from a cross-sectional study. Int J Equity Health. déc 2017;16(1):125. PubMed | Google Scholar
- Hajat C, Stein E. The global burden of multiple chronic conditions: a narrative review. Preventive Medicine Reports. 2018 Oct 19;12:284-293. PubMed | Google Scholar
- Burchell AN, Raboud J, Donelle J, Loutfy MR, Rourke SB, Rogers T et al. Cause-specific mortality among HIV-infected people in Ontario, 1995-2014: a population-based retrospective cohort study. CMAJO. 2019;7(1):E1-7. PubMed | Google Scholar
- Achwoka D, Waruru A, Chen TH, Masamaro K, Ngugi E, Kimani M et al. Noncommunicable disease burden among HIV patients in care: a national retrospective longitudinal analysis of HIV-treatment outcomes in Kenya, 2003-2013. BMC Public Health. 2019;19(1):372. PubMed | Google Scholar
- Pourcher G, Costagliola D, Martinez V. Obesity in HIV-infected patients in France: prevalence and surgical treatment options. Journal of Visceral Surgery. 2015;152(1):33-7. PubMed | Google Scholar
- Sawadogo A, Sanou S, Hema A, Kamboule BE, Kabore NF, Sore I et al. Metabolic syndrome and cardiovascular risk patients under antiretrovirals in a day hospital at Bobo-Dioulasso (Burkina Faso). Bull Soc Pathol Exot. 2014;107(3):151-8. PubMed | Google Scholar
- Tougouma JB, Yaméogo AA, Yaméogo NV, Hema A, Hien H, Kambiré Y et al. High rate of asymptomatic myocardial ischemia in HIV Infected population in Bobo-Dioulasso in Burkina Faso. Pan African Medical Journal. 2021;38. Google Scholar
- Mave V, Erlandson KM, Gupte N, Balagopal A, Asmuth DM, Campbell TB et al. Inflammation and change in body weight with antiretroviral therapy initiation in a multinational cohort of HIV-Infected adults. J Infect Dis. 2016;214(1):65-72. PubMed | Google Scholar
- Currier JS. Management of long-term complications of HIV disease: focus on cardiovascular disease. Top Antivir Med. 2018;25(4):133-7. PubMed | Google Scholar
- World Health Organization, Gilks C, Vitoria M. Antiretroviral therapy for HIV infection in adults and adolescents: recommendations for a public health approach. Geneva: World Health Organization. 2010. PubMed | Google Scholar
- World Health Organization. Rapid advice: antiretroviral therapy for HIV infection in adults and adolescents - November 2009. 2009;25. Google Scholar
- WHO. WHO publishes new clinical and service delivery recommendations for HIV prevention, treatment and care. Accessed May 23, 2022.
- Iwuji CC, Orne-Gliemann J, Larmarange J, Balestre E, Thiebaut R, Tanser F et al. Universal test and treat and the HIV epidemic in rural South Africa: a phase 4, open-label, community cluster randomised trial. The Lancet HIV. 2018;5(3):e116-25. PubMed | Google Scholar
- Moore DL, Allen UD. HIV in pregnancy: identification of intrapartum and perinatal HIV exposures. Paediatrics & Child Health. 2019;24(1):42-5. PubMed | Google Scholar
- Cohen MS, Chen YQ, McCauley M, Gamble T, Hosseinipour MC, Kumarasamy N et al. Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med. 2011;365(6):493-505. PubMed | Google Scholar
- Chas J, Hema A, Slama L, Kabore NF, Lescure FX, Fontaine C et al. The day-hospital of the university hospital, Bobo Dioulasso: an example of optimized HIV management in Southern Burkina Faso. Rouet F, éditeur. PLoS ONE. 2015;10(5):e0125588. PubMed | Google Scholar
- Ministry of Health, Burkina Faso. Report of the national survey on the prevalence of the main common risk factors for non-communicable diseases in Burkina Faso: STEPS survey. 2013;2014 Jun;104.
- Bakal DR, Coelho LE, Luz PM, Clark JL, De Boni RB, Cardoso SW et al. Obesity following ART initiation is common and influenced by both traditional and HIV-/ART-specific risk factors. Journal of Antimicrobial Chemotherapy. 2018;73(8):2177-85. PubMed | Google Scholar
- Kintu A, Liu E, Hertzmark E, Spiegelman D, Zack RM, Muya A et al. Incidence and risk factors for overweight and obesity after initiation of antiretroviral therapy in Dar es Salaam, Tanzania. J Int Assoc Provid AIDS Care. 2018 Jan-Dec;17:2325958218759759. PubMed | Google Scholar
- Koethe JR, Jenkins CA, Shepherd BE, Stinnette SE, Sterling TR. An optimal body mass index range associated with improved immune reconstitution among HIV-infected adults initiating antiretroviral therapy. Clinical Infectious Diseases. 2011;53(9):952-60. PubMed | Google Scholar
- Simo LP, Agbor VN, Temgoua FZ, Fozeu LCF, Bonghaseh DT, Mbonda AGN et al. Prevalence and factors associated with overweight and obesity in selected health areas in a rural health district in Cameroon: a cross-sectional analysis. BMC Public Health. 2021;21(1):475. PubMed | Google Scholar
- Debroy P, Sim M, Erlandson KM, Falutz J, Prado CM, Brown TT et al. Progressive increases in fat mass occur in adults living with HIV on antiretroviral therapy, but patterns differ by sex and anatomic depot. Journal of Antimicrobial Chemotherapy. 2019;74(4):1028-34. PubMed | Google Scholar
- Guehi C, Badjé A, Gabillard D, Ouattara E, Koulé SO, Moh R et al. High prevalence of being overweight and obese HIV-infected persons, before and after 24 months on early ART in the ANRS 12136 Temprano Trial. AIDS Research and Therapy. 2016 Feb 25;13:12. PubMed | Google Scholar
- Gogokhia L, Taur Y, Juluru K, Yagan N, Zhu YS, Pamer E et al. Intestinal dysbiosis and markers of systemic inflammation in viscerally and generally obese persons living with HIV. JAIDS Journal of Acquired Immune Deficiency Syndromes. 2020;83(1):81-9. PubMed | Google Scholar
- Yitbarek GY, Engidaw MT, Ayele BA, Tiruneh SA, Alamir MT. Magnitude of obesity/overweight and its associated factors among HIV/AIDS patients on antiretroviral therapy in Jimma Zone Hospitals, South West Ethiopia: hospital-based cross-sectional study. DMSO. 2020;13:1251-8. PubMed | Google Scholar
- Fezeu L, Minkoulou E, Balkau B, Kengne AP, Awah P, Unwin N et al. Association between socioeconomic status and adiposity in urban Cameroon. International Journal of Epidemiology. 2006;35(1):105-11. PubMed | Google Scholar
- Lopez RP. Neighborhood risk factors for obesity. Obesity. 2007;15(8):2111-9. PubMed | Google Scholar
- Shekar M, Popkin B. Obesity: health and economic consequences of an Impending global challenge. The World Bank. 2020. Google Scholar
- Hasse B, Iff M, Ledergerber B, Calmy A, Schmid P, Hauser C et al. Obesity trends and body mass index changes after starting antiretroviral treatment: the swiss HIV cohort study. Open Forum Infectious Diseases. 2014 Jul 1;1(2):ofu040. PubMed | Google Scholar
- Lakey W, Yang LY, Yancy W, Chow SC, Hicks C. Short communication: from wasting to obesity: initial antiretroviral therapy and weight gain in HIV-infected persons. AIDS Research and Human Retroviruses. 2013;29(3):435-40. PubMed | Google Scholar
- Barceló C, Guidi M, Thorball CW, Hammer C, Chaouch A, Scherrer AU et al. Impact of genetic and nongenetic factors on body mass index and waist-hip ratio change in HIV-infected individuals initiating antiretroviral therapy. Open Forum Infectious Diseases. 2020 Jan 22;7(1):ofz464. PubMed | Google Scholar
- Goupil de Bouillé J, Vigouroux C, Plessis L, Ghislain M, Teglas JP, Boufassa F et al. Factors associated with being overweight and obesity in people living with human immunodeficiency virus on antiretroviral therapy: socioclinical, inflammation, and metabolic markers. The Journal of Infectious Diseases. 2021;224(9):1570-80. PubMed | Google Scholar
- Koethe J, Jenkins C, Turner M, Bebawy S, Shepherd B, Wester C et al. Body mass index and the risk of incident noncommunicable diseases after starting antiretroviral therapy. HIV Medicine. 2015;16(1):67-72. PubMed | Google Scholar
- Givord P, Guillerm M, Multilevel models. Series of INSEE "statistical methodology" working papers. Working paper M. 2016/05.
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures

Article metrics

