Management of swallowed dental prosthesis impacting in cervical oesophagus: a six-month diagnostic delay (a case report)
Uchechukwu Chinelo Nze, Joseph Okwudili Ugwuanyi, Andrew Uzoma Ossai, Gloria Ogechukwu Ngwu, Basil Chukwuemeka Ezeanolue
Corresponding author: Joseph Okwudili Ugwuanyi, Department of Otolaryngology, University of Nigeria Teaching Hospital, Ituku Ozalla, Enugu State, Nigeria 
Received: 10 Apr 2026 - Accepted: 22 Apr 2026 - Published: 15 May 2026
Domain: Dental Public Health,Diagnostic radiology,Otolaryngology (ENT)
Keywords: Oesophagus, odynophagia, oesophagotomy, denture, case report
Funding: This work received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
©Uchechukwu Chinelo Nze et al. PAMJ Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Uchechukwu Chinelo Nze et al. Management of swallowed dental prosthesis impacting in cervical oesophagus: a six-month diagnostic delay (a case report). PAMJ Clinical Medicine. 2026;21:3. [doi: 10.11604/pamj-cm.2026.21.3.52660]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com//content/article/21/3/full
Case report 

Management of swallowed dental prosthesis impacting in cervical oesophagus: a six-month diagnostic delay (a case report)
Management of swallowed dental prosthesis impacting in cervical oesophagus: a six-month diagnostic delay (a case report)
![]() Uchechukwu Chinelo Nze1, Joseph Okwudili Ugwuanyi2,&, Andrew Uzoma Ossai2, Gloria Ogechukwu Ngwu2, Basil Chukwuemeka Ezeanolue2
Uchechukwu Chinelo Nze1, Joseph Okwudili Ugwuanyi2,&, Andrew Uzoma Ossai2, Gloria Ogechukwu Ngwu2, Basil Chukwuemeka Ezeanolue2
&Corresponding author
Foreign body impaction in the oesophagus requires emergency intervention. A focused history of the incident from the patient or caregiver usually provides the managing doctor with proper guidance in the course of care. Our patient´s case is so unique that he accidentally ingested his denture while taking a fish meal. This got impacted in the upper oesophagus, without him remembering the incident, as he attributed the pain he felt to the fish meal he had, leading to several months of misleading diagnosis of the cause of his odynophagia. Following careful history-taking and evaluation, a specialist otolaryngologist made a diagnosis of prolonged denture impaction in the oesophagus, six months after the incident. Denture was later safely extracted by oesophagotomy following failed oesophagoscopy as the oesophageal wall attempted to wall off the denture within its fibres; a rare natural attempt at preventing perforation and adjoining sequelae. Patient has recovered with marked improvement in swallowing and quality of life. A good clinical history remains indispensable in the evaluation and management of an impacted foreign body.

Impaction of swallowed objects in the oesophagus usually requires urgent, if not emergency treatment. Adult patients of sound mind will be aware of the incident and seek medical help soonest while in children, the care giver will be alarmed and also seek immediate medical help. This unusual case is that of an adult male of sound mind and body who accidentally swallowed his dental prosthesis but was not aware that it happened. This led to delays of definitive diagnosis and treatment for six months. The case is reported because of its rare queer clinical narratives and failure of many health practitioners, to diagnose the condition in a timely manner, despite available tools.

Patient information: a 60-year-old trader, was referred to Balsam Clinics, a specialist otorhinolaryngology clinic in Enugu, Nigeria, on account of difficulty with swallowing and pain at the lower right side of the neck of 6 months duration. Prior to presentation, the patient had a single flanged dental prosthesis at the upper left lateral incisor, which he had been using for several years without periodic dental maintenance. While eating a meal prepared with fish, he felt that a fish bone was stuck in his throat. He waited and hoped that the fish bone and pain would go away. After a few days, this pain persisted and progressed to painful difficulties in swallowing, but more to solids, and as such was sustaining himself on liquid meals. A few days after the fish meal incident, he could not find his dental prosthesis and proceeded to purchase a new replacement. He did not link the missing dental prosthesis to his odynophagia. A week into the onset of symptoms, he became worried that his symptoms worsened and decided to seek medical consultations. The first facility he went to did clinical and radiological evaluations. After plain radiographs of the neck and chest did not show a fish bone, a barium swallow was done as symptoms persisted. Again, he was told that there was no fish bone nor any other pathologies detected. They further did a flexible oesophagogastroduodenoscopy. The endoscopist reported “a difficult procedure. He found a hard, yellowish-white mass blocking the upper oesophageal sphincter.” He could not proceed beyond this spot. He diagnosed upper oesophageal neoplasia. He referred the patient to a cardiothoracic surgeon, but the patient declined to accept the referral. He sought a second opinion in two other facilities, one of which was a specialist Otolaryngologist. Each did plain radiographs and report normal findings with no impacted fish bone. They dismissed him with assurances that he will be symptom-free in a few days. It was not until the 6th month into his ordeal that he got a referral to another Otorhinolaryngology specialist clinic. Focused clinical history and physical examination done by this specialist led him to suspect impaction of a foreign body in the oesophagus that is bigger in size than a fish bone in a meal. This specialist then referred him to our Otorhinolaryngology specialty center for further management.
Clinical findings: on physical examination, he was clinically stable. There was point tenderness at the right side of the root of the neck, no obvious pooling of saliva, no palpable neck masses nor nodes. No other anomalies were detected in other regions.
Timeline of events: our patient presented to us on the 25th of June, 2025, with a six-month history of dysphagia and neck pain. Six months before presentation in December, 2024, he accidentally swallowed his denture (unaware he did) during a fish meal. He presented to two different hospitals between December, 2024 and March, 2025 on account of his dysphagia and pain, following which the exact diagnosis of impacted oesophageal foreign body could not be made on clinical, radiological, and endoscopic evaluation, leading to a diagnostic delay. As the symptoms persisted, he sought another opinion from a specialist otolaryngologist (one week before presentation), who referred him to our facility for definitive care. Upon presentation to us on 25th June, 2025, he was further evaluated clinically (including oesophagoscopy), and a magnetic resonance imaging (MRI) of the neck was done, which further suggested an impacted oesophageal foreign body.
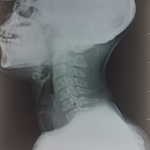
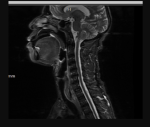
Diagnostic assessment: we recalled and reviewed the different radiological investigations done in the past six months. Some of the films showed obvious soft tissue shadow at C5-7 region (Figure 1), while others appeared unremarkable. He underwent rigid oesophagoscopy under general anaesthesia, during which the scope was noted to be difficult to pass through the cervical oesophagus at 16 cm from the upper central incisor. In fact, it met “a dead end” there was a mucosal bulge on the right side, just distal to the cricopharyngeus; no dental prosthesis was visualized at the oesophagoscopy. A decision was taken to abort the oesophagoscopy but to access the obstructing foreign body externally via a cervical oesophagotomy. As a precautionary measure, to evaluate the suggestion of oesophageal neoplasia made by the gastro-endoscopist, magnetic resonance imaging (MRI) was done (Figure 2). This excluded neoplasia and suggested foreign body impaction.
Therapeutic intervention: he had cervical oesophagotomy. The cervical oesophagus was approached from the right, through a transverse incision made along a skin crease from the midline to the anterior border of the sternocleidomastoid muscle, 4 cm above the sternal notch. Incision was deepened to the subplatysmal layer. The thyroid gland was retracted anteriorly, and sternocleidomastoid muscle with adjoining vascular structures were retracted posteriorly, exposing the tracheosophageal groove. A longitudinal incision was made into the right lateral side of the oesophageal muscle, (we opted for the right sided approach instead of the standard left-sided one because we determined the displacement of the dental prosthesis to the right side) extracting the dental prosthesis entangled completely within it, by carefully teasing out adherent muscle fibers “organizing” round the dental prosthesis (Figure 3). A size FG22 nasogastric feeding tube was passed. Oesophageal repair was done in layers using size 2/0 absorbable sutures. A passive drain was placed, and wound closed in layers. Post operatively, he was managed on analgesics, antibiotics, and fed via the NG tube.
Follow-up and outcome of intervention: he had a wound infection in the first week post-operatively, which was controlled by antibiotics. Skin sutures were removed on the 11th day post-op, following good healing, and graded oral feeding commenced. He has since commenced full oral intake, tolerating well, and has gone back to his job and routine.
Patient´s perspective: I would never have believed that I´ve had my denture for this long, lodged in my throat. That is why I kept going from one doctor to another for a solution to my pain on swallowing. Since the surgery, my throat has opened up and I can now swallow well.
Informed consent: the patient gave oral consent for the case to be published.
The impact of tooth loss and the associated desire to restore aesthetics has led to an increase in the number of people wearing dental prostheses [1]. Use of dental prosthesis improves facial aesthetics, makes eating pleasurable and enhances clarity of speech and communication. It has, therefore, been observed that edentulous people who wear dental prosthesis experience improved health and quality of life when compared to those without dental prosthesis [2]. However, such dental prosthesis may have their adverse effects when they dislodge and are accidentally swallowed. Factors predisposing to dental prosthesis dislodgement from the alveolus and impaction into the oesophagus include inappropriate size at fabrication, prolonged usage with its attendant wear and tear, and failure of its users in keeping appointments for dental clinic follow-up evaluations, especially when the dental prosthesis becomes unstable [1]. Our index patient has been using his dental prosthesis for several years without periodic dental maintenance, and that could have increased the risk of dislodgement. The prevalence of dental prosthesis impaction in the oesophagus has been reported to be higher in males than in females [3].
The majority of dental prostheses are made from poly(methyl methacrylate) (PMMA) plastics, which are radiolucent [4]. Radiolucency of dental prostheses is a well-documented cause for misdiagnosis and delayed treatment because this makes it difficult to use plain X-ray/radiograph, which is the most commonly used basic investigation for patients with suspected impacted oesophageal dental prosthesis, to directly confirm the diagnosis [4,5]. This could explain why the initial evaluation by a non-otorhinolaryngologist medical practitioner with the soft tissue X-ray of the neck done on the patient was missed. Also, focused clinical clerking was not conducted by the initial care provider. Good clinical evaluation eventually led to the correct diagnosis. Plain or contrast radiographs and flexible oesophago-gastroduodenoscopy were not substitutes for good clinical clerkmanship skills and physical examination competencies. Dental prosthesis ingestion has been reported to have a high misdiagnosis rate of 47% among patients with complaints of swallowed dental prosthesis [4].
Pre-operative localisation of impacted dental prosthesis in the oesophagus could be done with the tool of plain radiograph by looking not for the dental prosthesis to be directly demonstrated, but for the indirect signs in the plain radiograph films that have been reported to be fairly accurate [6]. These signs are the widening of the retro-tracheal/prevertebral region, indentation of the posterior trachea, and entrapped air column around the dental prostheses within the oesophagus [6]. The paper concluded that clinical history, physical examination, and plain soft tissue lateral neck radiographs were adequate for accurate diagnosis of impacted dental prosthesis in the cervical oesophagus [6]. These was utilized for accurate diagnosis in this index by one of the authors (BCE) from experience he reported and published previously [6].
Computerized tomographic (CT) scan and magnetic resonance imaging (MRI) are other available investigations that aid in the localization of impacted dental prosthesis in cases that are difficult to diagnose and localise its impacted site [3,5]. This patient had an MRI of the neck, not for diagnostic localisation but to rule out the possibility of neoplasia as suspected by a gastroenterologist's report following flexible oesophago-gastroduodenoscopy done on our index patient. The site of dental prosthesis impaction in the oesophagus is usually at the proximal area of constriction and the upper third of the oesophagus just below the cricopharyngeal junction [2,7]. Our patient also had his dental prosthesis impacted in the proximal oesophagus just 1cm below the cricopharyngeus. This is attributable to the rather peculiar nature of the dental prosthesis as a foreign body, which has serrated and irregular edges, and also because of its relatively large size. All these factors predispose to the impaction at the proximal area of constriction, and most of them may not slip further distally down the oesophagus [2]. Competent adults are normally able to give a clear history of foreign body ingestion and commonly complain of discomfort, dysphagia, odynophagia, retrosternal pain, sore throat, foreign body sensation, retching, and vomiting, which allows for prompt diagnosis and removal [4]. In some occasions, patients may receive treatment late because they presented late or because the diagnosis was earlier missed by the health care providers. The delayed scenarios may occur where the patient does not volunteer the history of ingestion of dental prosthesis, in demented and confused elderly patients [4]. Our patient was mentally competent, not confused, but was unaware that he accidentally swallowed the dental prosthesis. Once the correct diagnosis was confirmed, the best practice treatment was immediate removal of the dental prostheses from the oesophagus.
Further delay in removal predisposes to more complications [3,4,8]. Impaction time greater than twelve (12) hours is an independent factor associated with greater risk of complications, including perforation, ulceration, laceration, abscess, fistula, diverticulum, Horner's syndrome, and failure of retrieval [1,2,4,9]. This patient had a dental prosthesis impaction in the oesophagus for six (6) months before being successfully removed. This could be likened to a natural in vivo clinical experiment that would be unethical to carry out. At that point, the dental prosthesis can be best described as being deeply �buried´ and entangled within the oesophageal muscle wall, precluding its identification on rigid oesophagoscopy. The body tissue reactions were “organising” it within the musculature of the oesophagus. The oesophagus was not perforated, as often happens in this type of scenario. He escaped life-threatening complications probably because of this body's defense of walling the foreign object off. Mediastinitis was suspected by the radiologist, but we did not encounter it.
Visualisation and removal of impacted dental prosthesis in the oesophagus with a rigid oesophagoscope is very successful in most cases with minimal complications [6,9]. In difficult, complicated cases and failure of endoscopic retrieval, successful removal with open oesophagotomy has been variously reported and employed as an alternate route [1,2,6,10]. This index patient had cervical oesophagotomy and uneventful extraction of a 4cm single flanged denture following failure of diagnostic rigid oesophagoscopy to visualise it endoscopically for removal. Endoscopic retrieval was not attempted to forestall the exceedingly substantial risk of perforation posed in this case after the dental prosthesis had been impacted in the oesophagus for such a long period.
Competence and skill in clinical clerkship and physical examination are still essential tools for clinicians even in this era of advanced technology in medical diagnostic imaging and practice. We gained insight into the body´s natural defense response to walling off implanted oesophageal foreign bodies as evident in this patient´s oesophagus.
The authors declare no competing interests.
Uchechukwu Chinelo Nze operated on the patient, planned and wrote the case report, revised the manuscript, and approved the manuscript. Joseph Okwudili Ugwuanyi operated on the patient, planned and wrote the manuscript, revised and approved the manuscript. Andrew Uzoma Ossai operated on the patient, revised the manuscript, and approved the manuscript. Gloria Ogechukwu Ngwu took the operative photographs, revised the manuscript, and approved the manuscript. Basil Chukwuemeka Ezeanolue operated on the patient, planned and wrote the case report, wrote and revised the manuscript, and approved the manuscript. He supervised the other authors. All the authors have read and approved the final version of this manuscript.
We acknowledge the management of Balsam clinics, Enugu for providing the enabling environment for this patient to get the expert care needed. We also wish to thank the referring otolaryngologist who took his time to evaluate this patient clinically.
Figure 1: plain radiograph, neck lateral showing widening of the prevertebral space and anterior displacement of the trachea at the C5-7 levels
Figure 2: magnetic resonance imaging of the lower cervical oesophagus showing the impacted dental prosthesis
Figure 3: the extracted dental prosthesis
- Akinpelu OV, Amusa YB, Eziyi JA, Haastrup AA, Ameye SA. Oesophageal denture impaction producing Horner's syndrome: a case report. J Laryngol Otol. 2007;121(9):1-3. PubMed | Google Scholar
- Nwaorgu OG, Onakoya PA, Sogebi OA, Daniel D, Kokong DD, Dosumu OO. Esophageal Impacted Dentures. J Natl Med Assoc. 2004; 96(10):1350-1353. PubMed | Google Scholar
- Agrawal D, Lahiri TK, Parmar A, Sharma S. Swallowed Partial Dentures. Indian J dent Sc. 2012;4(2):7-12. Google Scholar
- Hashmi S, Walter J, Smith W, Latis S. Swallowed partial dentures. J R Soc Med. 2004 Feb;97(2):72-5. PubMed | Google Scholar
- Adedeji TO, Olaosun AO, Sogebi OA, Tobih JE. Denture Impaction in the Oesophagus Experience of a Young ENT Practice in Nigeria. Pan Afr Med J. 2014 Aug 25;18:330. PubMed | Google Scholar
- Ezeanolue BC. Localisation and removal of swallowed radiolucent dental prostheses impacted in cervical oesophagus. International Journal of Medicine and Health Development. 1999 Jan 1;4(1):46-50. Google Scholar
- Ahmad M, Abubakar Y. Pharyngo-oesophageal Foreign Bodies in Maiduguri. The Nigerian Journal of Surgical Research. 2001;3(2):62-65. Google Scholar
- Tihan D, Trabulus D, Altunkay A, Karaca S, Cihan A, Alis H. Esophageal perforation due to inadvertent swallowing of a dental prosthesis. Turk J Gastroenterol. 2011;22(5):529-533. PubMed | Google Scholar
- Hong KH, Kim YJ, Kim JH, Chun SW, Kim HM, Cho JH. Risk factors for complications associated with upper gastrointestinal foreign bodies. World J Gastroenterol. 2015 Jul 14;21(26):8125-31. PubMed | Google Scholar
- Shreshtha D, Sikka K, Singh CA, Thakar A. Foreign body esophagus: when endoscopic removal fails. Indian J Otolaryngol Head Neck Surg. 2013 Dec;65(4):380-2. PubMed | Google Scholar
Search

This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures


Article metrics
Recently from the PAMJ-CM