

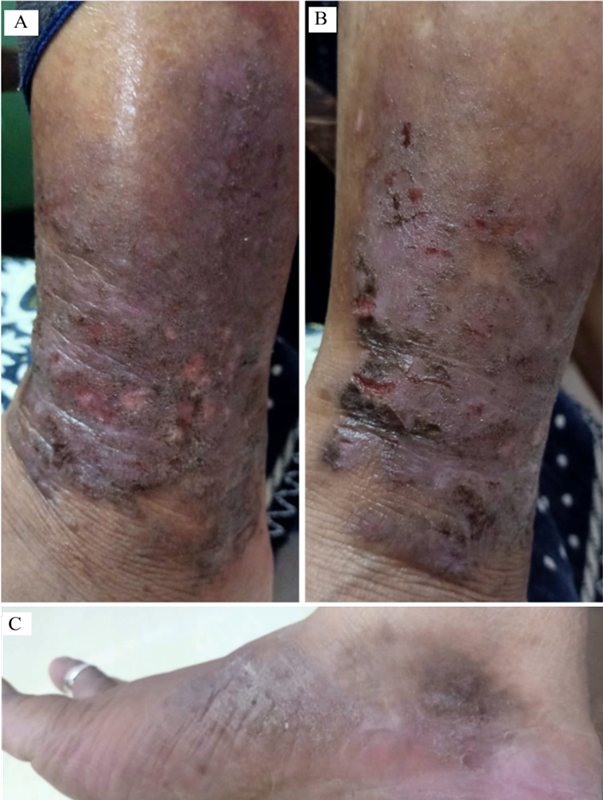
Refractory grade III atopic dermatitis of the extremities in a post-menopausal female
Aditi Satish Telrandhe, Anita Santoshrao Wanjari
PAMJ-CM. 2026; 20:17. Published 25 Mar 2026 | doi:10.11604/pamj-cm.2026.20.17.49691
Corresponding author
Anita Santoshrao Wanjari, Department of Rasashastra Evam Bhaishajya Kalpana, Mahatma Gandhi Ayurveda Collage Hospital and Research Center, Datta Meghe Institute of Higher Education and Research Salod (H) Wardha, Maharashtra, India (anitawanjari7@gmail.com)
This image
| Articles published in PAMJ-CM are Open Access and distributed under the terms of the Creative Commons Attribution 4.0 International (CC BY 4.0). |  |

eISSN: 2707-2797
The PAMJ Clinical Medicine (ISSN: 2707-2797) is a subsidiary of the Pan African Medical Journal. The contents of this journal is intended exclusively for professionals in the medical, paramedical and public health and other health sectors.
Currently tracked by: DOAJ, AIM, Google Scholar, AJOL, EBSCO, Scopus, Embase, IC, HINARI, Global Health, PubMed Central, PubMed/Medline, ESCI
Physical address: Kenya: 3rd Floor, Park Suite Building, Parkland Road, Nairobi. PoBox 38583-00100, tel: +254 (0)20-520-4356 | Cameroon: Immeuble TechnoPark Essos, Yaounde, PoBox: 10020 Yaounde, tel: +237 (0)24-309-5880

About PAMJ - Manuscript Hut™
The Manuscript Hut is a product of the PAMJ Center for Public health Research and Information.
Kenya: 3rd Floor, Park Suite Building, Parkland Road, Nairobi. PoBox 38583-00100, tel: +254 (0)20-520-4356
Cameroon: Immeuble TechnoPark Essos, Yaounde, PoBox: 10020 Yaounde, tel: +237 (0)24-309-5880
Copyright © - Pan African Medical Journal - CEPHRI. 2026
Haraka Publishing Platform - (MMS V.2.5). Release date Jan 2018 - Customized for PAMJ - Clinical Medicine
services@panafrican-med-journal.com
 |