
Management of a degenerated fundal leiomyoma mimicking an adnexal mass on ultrasound in a postmenopausal patient: a case report
Naoufal El Harbili, Saad Benali, Moulay El Mehdi El Hassani, Jaouad Kouach
Corresponding author: Naoufal El Harbili, Department of Gynecology-Obstetrics, Military Hospital of Instruction Mohamed V, Rabat, Morocco 
Received: 21 Apr 2026 - Accepted: 13 May 2026 - Published: 23 Jun 2026
Domain: Obstetrics and gynecology
Keywords: Leiomyoma, uterine fibroid, cystic degeneration, laparoscopy, case report
Funding: This work received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
©Naoufal El Harbili et al. PAMJ Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Naoufal El Harbili et al. Management of a degenerated fundal leiomyoma mimicking an adnexal mass on ultrasound in a postmenopausal patient: a case report. PAMJ Clinical Medicine. 2026;21:13. [doi: 10.11604/pamj-cm.2026.21.13.52910]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com//content/article/21/13/full
Case report 

Management of a degenerated fundal leiomyoma mimicking an adnexal mass on ultrasound in a postmenopausal patient: a case report
Management of a degenerated fundal leiomyoma mimicking an adnexal mass on ultrasound in a postmenopausal patient: a case report
![]() Naoufal El Harbili1,2,&,
Naoufal El Harbili1,2,&, ![]() Saad Benali1,2,
Saad Benali1,2, ![]() Moulay El Mehdi El Hassani1,2, Jaouad Kouach1,2
Moulay El Mehdi El Hassani1,2, Jaouad Kouach1,2
&Corresponding author
Uterine leiomyomas represent the most common pelvic tumors in women of reproductive age; however, their persistence or de novo diagnosis in postmenopausal women remains uncommon and frequently raises diagnostic challenges. Cystic degeneration of a fundal myoma can result in a complex cystic pelvic mass that closely mimics an adnexal lesion on conventional ultrasound, thereby leading to erroneous preoperative classification. We report the case of a 60-year-old postmenopausal patient who presented with chronic pelvic pain evolving over six months. Pelvic ultrasonography revealed a median para-uterine cystic mass measuring 9.5cm — 7.8cm — 6.2cm, interpreted as most likely of adnexal origin. Tumor marker CA-125 was within the normal range at 18 U/mL. Exploratory laparoscopy revealed a pedunculated fundal leiomyoma classified as FIGO type 6, exhibiting cystic degeneration, with macroscopically normal bilateral adnexa. Total hysterectomy with bilateral salpingo-oophorectomy was performed. Histopathological examination confirmed a benign leiomyoma in hyaline-cystic degeneration. The postoperative course was uneventful, with complete pain resolution at six-month follow-up. This observation underscores the diagnostic pitfalls inherent to degenerative myomas in postmenopausal women and highlights the critical role of exploratory laparoscopy in resolving diagnostic uncertainty before definitive surgical management.

Uterine leiomyomas are benign smooth muscle tumors that represent the most frequent pelvic neoplasms among women of reproductive age, with an estimated prevalence ranging from 20% to 40% [1]. Their biological behavior is largely governed by sex steroid hormones, and spontaneous regression is classically expected following the cessation of ovarian activity at menopause. Nevertheless, symptomatic leiomyomas persisting beyond menopause — or presenting for the first time in this life period — are well-documented, albeit infrequent, clinical occurrences [2]. Degenerative changes within myomas are encountered in approximately 65% of cases at histological examination, with hyaline degeneration constituting the most prevalent form, followed by cystic, red (carneous), and calcific variants [3]. Cystic degeneration, in particular, results in the liquefaction of the central myomatous tissue, producing anechoic or hypoechoic cavities that may be indistinguishable from ovarian cysts or complex adnexal masses on pelvic ultrasonography [4]. This imaging ambiguity is further amplified in postmenopausal patients, where the clinical suspicion of an ovarian neoplasm necessarily rises given the higher malignant potential associated with adnexal masses in this age group [5]. In this case report, we present the unusual clinical history of a 60-year-old postmenopausal female who presented with a large fundal leiomyoma in cystic degeneration, initially misidentified as an adnexal mass on ultrasound, and discuss the diagnostic and therapeutic management of this deceptive condition.

Patient information: we present the case of a 60-year-old patient, G3P3, menopausal for five years, who was referred to our department for chronic pelvic pain with progressive onset evolving over six months. Her past medical history was notable for controlled arterial hypertension under single-agent therapy. Her gynecological and obstetric history was unremarkable, with no prior pelvic surgery, no history of long-term oral contraceptive use, and no menopausal hormone therapy. The patient reported no abnormal uterine bleeding, urinary symptoms, or constitutional signs.
Clinical findings: general examination on admission revealed a hemodynamically stable patient: blood pressure 132/78 mmHg, heart rate 78 bpm, SpO2 98% on room air, weight 60 kg, height 1.65 m, and body mass index (BMI) of 22 kg/m2. Abdominopelvic examination identified a palpable suprapubic pelvic mass, adherent to the uterus, associated with pain on uterine mobilization. No latero-uterine mass was detected. The remainder of the physical examination was normal.
Timeline: the patient first consulted on day 0 for chronic pelvic pain evolving over six months, prompting a clinical examination and the ordering of imaging and biological investigations. On day 1, pelvic ultrasonography identified a para-uterine cystic mass measuring 9.5 ×7.8 ×6.2 cm of suspected adnexal origin, with a CA-125 level of 18 U/mL; following multidisciplinary discussion, the decision was made to proceed with exploratory laparoscopy. On day 7, intraoperative findings revealed a pedunculated fundal myoma FIGO type 6 in cystic degeneration with macroscopically normal bilateral adnexa, leading to the decision to perform a total hysterectomy with bilateral salpingo-oophorectomy; the patient was discharged uneventfully on postoperative day 3. At week 4, the anatomopathological report confirmed a benign leiomyoma in hyaline-cystic degeneration, which was communicated to the patient. At the six-month follow-up consultation, the patient reported complete resolution of pelvic pain with no evidence of recurrence (Table 1).
Diagnostic assessment: pelvic ultrasonography revealed a median para-uterine cystic mass measuring 9.5 × 7.8 × 6.2 cm, with regular borders and anechoic content, predominantly interpreted as being of adnexal origin. Serum CA-125 was measured at 18 μ/mL, within the normal reference range. No additional cross-sectional imaging was performed preoperatively given the ultrasound findings and the clinical decision to proceed with diagnostic laparoscopy. The initial differential diagnosis included a mucinous or serous ovarian cystadenoma, a paraovarian cyst, or a degenerative uterine myoma; however, the ultrasound characteristics, in the absence of a visible uterine pedicle, favored an adnexal origin.
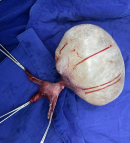
Therapeutic interventions: under general anesthesia, an exploratory laparoscopy was performed. Peroperative findings revealed a uterus of normal size for age, bilaterally normal adnexa, and a large pedunculated fundal mass arising from the uterine fundus, consistent with a FIGO type 6 leiomyoma exhibiting gross cystic degeneration. Given these intraoperative findings, the decision was made to proceed with total hysterectomy with bilateral salpingo-oophorectomy via median laparotomy. The surgical specimen was sent in its entirety for anatomopathological analysis. The mass presented as a single lesion measuring approximately 9.5 × 7.8 × 6.2 cm, with a smooth pearlescent surface consistent with underlying cystic degeneration, illustrating its capacity to mimic an adnexal mass on preoperative ultrasound (Figure 1). No peritoneal implants, ascites, or abnormal lymphadenopathy were identified.
Follow-up and outcome: the postoperative course was uneventful. The patient was discharged on postoperative day three in satisfactory general condition. Histopathological examination of the surgical specimen confirmed the diagnosis of a benign uterine leiomyoma displaying hyaline-cystic degeneration, with no histological features of malignancy, no mitotic activity, and clear surgical margins. During the follow-up consultation conducted at six months post-surgery, the patient reported complete resolution of the chronic pelvic pain that had motivated her initial presentation. No evidence of recurrence or new pelvic complaints was noted at that stage.
Patient perspective: the patient expressed initial concern upon learning that a large pelvic mass had been discovered, with particular anxiety regarding the possibility of a malignant ovarian tumor. The prospect of exploratory surgery was accepted after thorough information and shared decision-making with the surgical team. Following the operation and the benign histopathological confirmation, the patient reported significant psychological reassurance alongside the resolution of her chronic pain. She expressed satisfaction with the overall management and showed strict adherence to postoperative follow-up.
Informed consent: written informed consent was obtained from the patient for the publication of this anonymized case report and the accompanying intraoperative image. The signed consent form is held in the patient's hospital record.
Epidemiological aspects: uterine fibroids affect between 20% and 40% of women of reproductive age, yet their occurrence in the postmenopausal setting is markedly less frequent, estimated at approximately 10-15% of cases referred for pelvic mass evaluation in this population [6]. In our case, the discovery of a large symptomatic leiomyoma in a 60-year-old patient menopausal for five years represents an atypical clinical scenario that underscores the fact that myoma regression following menopause is neither universal nor predictable. The absence of exogenous hormonal exposure in our patient further underscores the role of other contributing factors, including local paracrine mechanisms and adipose tissue-derived estrogen production.
Pathophysiological aspects: degenerative changes within leiomyomas are the result of inadequate blood supply relative to the tumor's metabolic demands. Among the recognized subtypes, hyaline degeneration — characterized by replacement of smooth muscle cells by acellular collagen — is the most prevalent, occurring in up to 60% of specimens [3]. Cystic degeneration, as observed in our patient, arises from liquefaction of hyalinized areas, resulting in fluid-filled cavities that may simulate ovarian cysts or paraovarian structures on imaging. Furthermore, in postmenopausal women, the natural vascular rarefaction of myomatous tissue may accelerate this cystic transformation, contributing to diagnostic confusion.
Clinical and diagnostic aspects: the classical clinical presentation of uterine fibroids — abnormal uterine bleeding, pelvic pressure, and dysmenorrhea — is seldom encountered in postmenopausal patients, where the dominant symptom tends to be pelvic pain or pressure secondary to mass effect. In our case, the patient's primary complaint was chronic pelvic pain for over six months without vaginal bleeding, consistent with the published literature on postmenopausal myomas [7]. Pelvic ultrasound remains the first-line imaging modality in the evaluation of pelvic masses; however, its accuracy in differentiating a degenerated pedunculated myoma from an adnexal mass is considerably limited when the lesion has lost its characteristic echographic features. In our patient, the absence of a visible uterine pedicle on initial ultrasound led to the erroneous classification of the mass as adnexal in origin — a well-recognized diagnostic pitfall [4].
Differential diagnosis: the principal differential diagnoses considered in this postmenopausal patient with a cystic pelvic mass included serous and mucinous ovarian cystadenoma, ovarian borderline tumor, paraovarian cyst, and peritoneal inclusion cyst. The normal serum CA-125 level (18 μ/mL) provided some reassurance against an epithelial ovarian malignancy, although the limitations of this biomarker in distinguishing benign from malignant adnexal masses are well established — its sensitivity for early-stage disease being particularly insufficient [5]. It is worth mentioning that magnetic resonance imaging (MRI) of the pelvis could have potentially clarified the uterine origin of the mass preoperatively; however, the clinical decision to proceed directly to diagnostic laparoscopy was deemed appropriate given the constellation of findings and the need for simultaneous therapeutic management.
Therapeutic and prognostic aspects: the management of a pelvic mass in a postmenopausal patient must integrate the diagnostic uncertainty, the malignancy risk profile, and the symptomatic burden. In our case, exploratory laparoscopy provided simultaneous diagnostic clarification and the opportunity for immediate definitive surgery. Total hysterectomy with bilateral salpingo-oophorectomy was elected as the definitive procedure, consistent with current recommendations for symptomatic uterine pathology in postmenopausal patients without fertility considerations [8]. This approach eliminated the risk of undiagnosed coexisting ovarian pathology and provided the specimen for complete histological characterization. The confirmation of a purely benign leiomyoma in hyaline-cystic degeneration — with no sarcomatous features — was a critical outcome, given the low but non-negligible risk of leiomyosarcoma estimated at 0.1-0.3% in surgical series [9]. In our case, the diagnostic trajectory — from an ultrasound-suspected adnexal mass to an intraoperatively confirmed pedunculated uterine myoma — illustrates the limitations of non-invasive imaging in distinguishing extruded pedunculated fibroids from ovarian neoplasms [10]. Our observation reinforces the value of systematic intraoperative exploration of all pelvic structures, including careful identification of the bilateral adnexa, before any irreversible surgical decision. Furthermore, the absence of uterine connection to the cystic mass on ultrasound should not, on its own, exclude a myomatous etiology when clinical and biological parameters remain reassuring.
Degenerative uterine leiomyomas in postmenopausal women represent an uncommon but clinically significant entity capable of closely mimicking adnexal pathology on pelvic ultrasonography. The cystic transformation of a pedunculated fundal fibroid — as illustrated by this observation — carries a high risk of diagnostic misclassification, with potential consequences for preoperative planning and surgical strategy. Exploratory laparoscopy remains an invaluable tool in resolving diagnostic uncertainty, allowing simultaneous identification and definitive management of the pelvic mass. Total hysterectomy with bilateral salpingo-oophorectomy constitutes the treatment of choice in postmenopausal patients, ensuring both symptomatic relief and complete histological characterization of the specimen. Patients presenting with a pelvic mass in the postmenopausal period require individualized multidisciplinary management to ensure optimal diagnostic accuracy and therapeutic outcomes.
The authors declare no competing interests.
Naoufal El Harbili wrote the article, designed the project, analyzed the data, and contributed to the discussion. Saad Benali, Moulay El Mehdi El Hassani, and Jaouad Kouach treated the patient, gathered the patient's information, and supervised the project. All authors have read and approved the final version of this manuscript.
Table 1: CARE timeline — clinical course of the degenerated fundal leiomyoma case
Figure 1: surgical specimen after total hysterectomy with bilateral salpingo-oophorectomy for a FIGO type 6 pedunculated fundal leiomyoma in cystic degeneration (HMI Mohamed V, Rabat, Morocco, 2024); single lesion, smooth pearlescent surface, bilateral adnexa macroscopically normal
- Baird DD, Dunson DB, Hill MC, Cousins D, Schectman JM. High cumulative incidence of uterine leiomyoma in black and white women: ultrasound evidence. Am J Obstet Gynecol. 2003;188(1):100-107. PubMed | Google Scholar
- Pollow K, Geilfuss J, Boquoi E, Pollow B. Estrogen and progesterone binding proteins in normal human myometrium and leiomyoma tissue. J Clin Chem Clin Biochem. 1978;16(9):503-511. PubMed | Google Scholar
- Murase E, Siegelman ES, Outwater EK, Perez-Jaffe LA, Tureck RW. Uterine leiomyomas: histopathologic features, MR imaging findings, differential diagnosis, and treatment. Radiographics. 1999;19(5):1179-1197. PubMed | Google Scholar
- Exacoustos C, Romanini ME, Amadio A, Amoroso C, Szabolcs B, Zupi E et al. Can gray-scale and color Doppler sonography differentiate between uterine leiomyosarcoma and leiomyoma. J Clin Ultrasound. 2007;35(8):449-457. PubMed | Google Scholar
- Jacobs I, Oram D, Fairbanks J, Turner J, Frost C, Grudzinskas JG. A risk of malignancy index incorporating CA 125, ultrasound and menopausal status for the accurate preoperative diagnosis of ovarian cancer. Br J Obstet Gynaecol. 1990;97(10):922-929. PubMed | Google Scholar
- Laughlin SK, Baird DD, Savitz DA, Herring AH, Hartmann KE. Prevalence of uterine leiomyomas in the first trimester of pregnancy. Obstet Gynecol. 2009;113(3):630-635. PubMed | Google Scholar
- Okolo S. Incidence, aetiology and epidemiology of uterine fibroids. Best Pract Res Clin Obstet Gynaecol. 2008;22(4):571-588. PubMed | Google Scholar
- Stovall TG. Hysterectomy. In: Berek JS, ed. Berek and Novak's Gynecology. 15th ed. Lippincott Williams & Wilkins; 2012:725-755.
- Leibsohn S, d'Ablaing G, Mishell DR Jr, Schlaerth JB et al. Leiomyosarcoma in a series of hysterectomies performed for presumed uterine leiomyomas. Am J Obstet Gynecol. 1990;162(4):968-976. PubMed | Google Scholar
- Parker WH, Fu YS, Berek JS. Uterine sarcoma in patients operated on for presumed leiomyoma and rapidly growing leiomyoma. Obstet Gynecol. 1994;83(3):414-418. PubMed | Google Scholar
Search

This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures
Article metrics
Recently from the PAMJ-CM






