
Large subserosal fundal fibroid with cystic degeneration causing incomplete uterine torsion in a 65-year-old postmenopausal woman: a case report
El Harbili Naoufal, Benali Saad, El Hassani Moulay El Mehdi, Kouach Jaouad
Corresponding author: El Harbili Naoufal, Department of Gynecology-Obstetrics, Mohammed V Military University Hospital, Faculty of Medicine and Pharmacy, Mohammed V University, Rabat, Morocco 
Received: 22 Apr 2026 - Accepted: 28 May 2026 - Published: 07 Jul 2026
Domain: Obstetrics and gynecology
Keywords: Uterine torsion, uterine fibroid, cystic degeneration, postmenopausal, hysterectomy, case report
Funding: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
©El Harbili Naoufal et al. PAMJ Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: El Harbili Naoufal et al. Large subserosal fundal fibroid with cystic degeneration causing incomplete uterine torsion in a 65-year-old postmenopausal woman: a case report. PAMJ Clinical Medicine. 2026;21:16. [doi: 10.11604/pamj-cm.2026.21.16.52934]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com//content/article/21/16/full
Case report 

Large subserosal fundal fibroid with cystic degeneration causing incomplete uterine torsion in a 65-year-old postmenopausal woman: a case report
Large subserosal fundal fibroid with cystic degeneration causing incomplete uterine torsion in a 65-year-old postmenopausal woman: a case report
![]() El Harbili Naoufal1,&,
El Harbili Naoufal1,&, ![]() Benali Saad1,
Benali Saad1, ![]() El Hassani Moulay El Mehdi1, Kouach Jaouad1
El Hassani Moulay El Mehdi1, Kouach Jaouad1
&Corresponding author
Uterine torsion is a rare and potentially life-threatening gynaecological emergency defined by rotation of the uterus greater than 45° on its longitudinal axis. Giant subserosal leiomyomas with cystic degeneration represent a recognised precipitating factor, yet their occurrence in postmenopausal women remains exceptional. We report the case of a 65-year-old postmenopausal patient presenting with a two-month history of progressive abdominopelvic heaviness and intermittent pelvic pain, in whom pelvic magnetic resonance imaging (MRI) revealed a subserosal fundal leiomyoma measuring 24x22x15 cm with extensive cystic degeneration and a solid component of 82x44x95 mm, responsible for an incomplete uterine torsion on the vertical axis. Biological work-up demonstrated a haemoglobin of 11.2 g/dL, C-reactive protein of 48 mg/L, and CA-125 of 38 U/mL; endometrial biopsy confirmed atrophic endometrium. The patient underwent total abdominal hysterectomy with bilateral salpingo-oophorectomy (TAH-BSO); estimated blood loss was 650 mL and the surgical specimen weighed 5.2 kg. Histopathological examination confirmed a benign leiomyoma with hyaline and cystic degeneration, devoid of sarcomatous transformation. The postoperative course was uneventful; the patient was discharged on day 3 and remained symptom-free at the six-week follow-up. This observation underscores the diagnostic challenge posed by giant degenerating fibroids in postmenopausal women and highlights the necessity of timely surgical intervention to prevent irreversible complications.

Uterine torsion is an uncommon gynaecological condition characterised by rotation of the uterus greater than 45° around its longitudinal axis, most frequently precipitated by large structural uterine anomalies [1]. Two principal forms are distinguished: complete torsion (rotation ≥ 180°), which constitutes a surgical emergency due to the risk of vascular occlusion and uterine necrosis; and incomplete torsion (<180°), which may follow a more insidious clinical course, thereby increasing the risk of delayed diagnosis [2].
Uterine leiomyomas are the most frequent benign tumours of the female genital tract, affecting up to 70-80% of women by the age of 50 [3,4]. Although fibroid regression is classically anticipated after the menopause, a non-negligible proportion of postmenopausal patients harbour large or symptomatic fibroids, occasionally complicated by degenerative changes. Cystic degeneration - resulting from central liquefactive necrosis - substantially increases tumour mass and distorts uterine anatomy, further predisposing to torsion [5].
The occurrence of uterine torsion in a postmenopausal patient is genuinely exceptional, with fewer than fifty cases documented in the world literature [6]. This report aims to present a case of incomplete uterine torsion secondary to a giant subserosal fundal leiomyoma with cystic degeneration in a 65-year-old postmenopausal woman, and to discuss the diagnostic and therapeutic approaches appropriate for this presentation.

Patient information
A 65-year-old postmenopausal woman (G4P4, BMI 27 kg/m²) was referred to our department for a two-month history of progressive abdominopelvic heaviness, increasing abdominal circumference, and intermittent pelvic pain. Menopause had been established at age 51 without hormonal replacement therapy. Her sole medical history was well-controlled stage I essential hypertension managed with Amlodipine 5 mg once daily. No prior gynaecological surgery had been performed and there was no family history of gynaecological malignancy.
Clinical findings
On admission, the patient was haemodynamically stable: blood pressure 128/76 mmHg, heart rate 86 beats/min, respiratory rate 18 cycles/min, and temperature 378�C. Abdominal examination revealed marked distension with a firm, tender, non-mobile pelvic mass extending to the umbilical level. On pelvic examination, the cervix maintained its normal anatomical position. No lymphadenopathy was identified.
Timeline
Over the two months preceding admission, the patient experienced progressive pelvic heaviness and abdominal distension, prompting an outpatient referral following an ultrasound demonstrating a large heterogeneous fundal mass. On admission (day 1), acute pelvic pain, nausea, and malaise were the leading complaints, and biological and imaging work-up was initiated. Pelvic MRI obtained on day 3 confirmed incomplete uterine torsion, leading to a decision for elective laparotomy. Preoperative optimisation was completed by day 5. Surgery was performed on day 6, and the patient was discharged on postoperative day 3. At the six-week outpatient follow-up, she was completely asymptomatic (Table 1).
Diagnostic assessment
Laboratory work-up demonstrated: haemoglobin 11.2 g/dL, white blood cell count 12.4x109/L, C-reactive protein 48 mg/L, and CA-125 38 U/mL - mildly elevated but consistent with the mass effect of a large fibroid rather than malignancy [7]. CA 19-9, thyroid function, and coagulation studies were within normal limits. Endometrial biopsy confirmed atrophic endometrium with no atypia. Pelvic MRI - performed in the three planes of space using T1, T2 Fat Sat, and T1 Fat Sat sequences with paramagnetic contrast injection, complemented by diffusion-weighted imaging - identified a large subserosal fundal uterine mass, well delineated, measuring 24x15x22 cm, with T1 hypointensity, T2 hyperintensity, and extensive cystic degeneration. A solid component measuring 82x44x95 mm was present, demonstrating T1/T2 hypointensity, no restricted diffusion, and contrast enhancement identical to the adjacent myometrium - findings arguing strongly against sarcomatous transformation. Crucially, MRI confirmed an incomplete torsion of the uterus on its vertical axis secondary to this mass (Figure 1, Figure 2, Figure 3). The endometrium was thin and homogeneous; both ovaries were atrophic; a small peritoneal effusion was present; no lymphadenopathy was identified. The radiological conclusion was unambiguous: a voluminous type-7 subserosal fundal leiomyoma with extensive cystic degeneration responsible for incomplete uterine torsion (Figure 4) [8].
Therapeutic interventions
Following multidisciplinary discussion, a decision was made for elective total abdominal hysterectomy with bilateral salpingo-oophorectomy (TAH-BSO). Under general anaesthesia via midline laparotomy, intraoperative exploration confirmed a 90° anticlockwise incomplete uterine rotation. The subserosal fundal mass (24x22 cm) had a smooth, non-ruptured surface; both adnexae were atrophic; a small serous peritoneal effusion was present. Following careful de-rotation of the uterus, TAH-BSO was completed without incident. Estimated blood loss was 650 mL, requiring one unit of packed red blood cells intraoperatively. The surgical specimen weighed 5.2 kg.
Follow-up and outcomes
The postoperative period was uneventful. The patient was mobilised on Day 1 and resumed oral feeding the same day. She was discharged on postoperative Day 3 under oral analgesics and subcutaneous enoxaparin 40 mg once daily for 14 days. Histopathological examination of the surgical specimen confirmed a benign leiomyoma with extensive hyaline and cystic degeneration; no coagulative-type necrosis, significant nuclear atypia, or elevated mitotic index (<5 mitoses per 10 high-power fields) was identified, firmly excluding leiomyosarcoma [9]. At the six-week outpatient follow-up, the patient was completely asymptomatic with no residual pelvic complaints and no wound complications.
Patient perspective
The patient consented to publication and reported that the two months preceding diagnosis were marked by progressive abdominal enlargement she had initially attributed to weight gain. The acute pain episode that precipitated hospitalisation was described as frightening and unexpected. She expressed considerable relief on learning of the benign histological outcome and wished to convey, for the benefit of other postmenopausal women, that gynaecological symptoms should not be minimised on the assumption that fibroid disease invariably resolves after the menopause.
Informed consent
Written informed consent for the publication of this case report, including clinical data and imaging, was obtained from the patient prior to submission. The original signed consent document is held in the patient's medical file at Mohammed V Military University Hospital (HMI Mohamed V), Rabat, Morocco.
Uterine torsion remains among the most rarely reported gynaecological emergencies, distinguished from ovarian torsion by its predilection for structural uterine anomalies rather than adnexal pathology [1,6]. The present observation is instructive at several levels: it involves a postmenopausal patient in whom leiomyoma persistence is itself atypical; the causative tumour had reached a surgical weight of 5.2 kg with extensive cystic degeneration; and the torsion was incomplete, producing a clinical presentation sufficiently insidious to have been tolerated over two months before prompting hospitalisation.
Pathophysiology
The mechanical basis of uterine torsion rests upon asymmetric distribution of mass around the uterine longitudinal axis, combined with laxity of the supporting ligamentous structures [2]. Subserosal fundal fibroids generate a lever-arm effect proportional to their size and eccentricity. The additional mass conferred by extensive cystic degeneration further increased this tumour's propensity to shift the uterine centre of gravity. Furthermore, postmenopausal atrophy of the pelvic floor musculature likely reduced the structural threshold for torsion compared with a premenopausal patient of equivalent fibroid size.
Fibroid persistence and cystic degeneration in the postmenopause
Although oestrogen withdrawal at the menopause is expected to induce fibroid involution, this process is incomplete in a subset of patients, particularly those with larger tumours [4,5]. Cystic degeneration substantially increases diagnostic complexity, as large cystic fibroids may closely mimic adnexal masses or, most critically in a postmenopausal context, cystic ovarian malignancy. In our case, the absence of restricted diffusion in the solid component, the enhancement pattern identical to the myometrium, and the atrophic adnexa collectively argued against malignancy on MRI.
Role of MRI
The mildly elevated CA-125 (38 U/mL) - a well-recognised non-specific finding in the context of large fibroids and peritoneal irritation [7] - combined with a giant postmenopausal pelvic mass, created a genuine diagnostic dilemma. Pelvic MRI proved indispensable not only in characterising the fibroid and excluding malignancy, but specifically in demonstrating the incomplete uterine rotation on sagittal and coronal sequences, a finding virtually impossible to characterise on ultrasound alone [8]. Awareness of uterine torsion as a differential diagnosis is therefore a prerequisite for its inclusion in the MRI interpretation request.
Surgical strategy and exclusion of leiomyosarcoma
In this postmenopausal patient, TAH-BSO represented the unambiguous surgical choice. Although leiomyosarcoma accounts for less than 1% of uterine malignancies, its preoperative exclusion is critical in postmenopausal patients with rapidly enlarging, degenerating fibroids [9,10]. Neither MRI nor serum markers provide sufficient specificity to definitively exclude sarcomatous transformation preoperatively; the definitive diagnosis belongs exclusively to histopathological analysis, which confirmed benign disease in our case.
Limitations
The retrospective single-case design and the six-week follow-up period limit broader generalisability. The unavailability of molecular or immunohistochemical data precludes further characterisation of the degenerative process. Nevertheless, this observation contributes to a well-documented, imaging-confirmed, histopathologically validated example of an exceptionally rare clinical entity.
Giant subserosal uterine fibroids with cystic degeneration may precipitate incomplete uterine torsion even in postmenopausal women - a clinical setting in which such pathology is neither routinely anticipated nor easily recognised. Pelvic MRI is the cornerstone imaging modality for confirming the diagnosis, characterising the fibroid, and excluding malignancy. Total abdominal hysterectomy with bilateral salpingo-oophorectomy, preceded by careful preoperative optimisation and confirmed by histopathological analysis, constitutes definitive management in postmenopausal patients with this presentation. Giant uterine fibroids with degenerative changes in postmenopausal women require special attention, multidisciplinary evaluation, and timely surgical intervention to prevent irreversible complications.
The authors declare no competing interests.
El Harbili Naoufal wrote the article, designed the project, analysed the data, and contributed to the discussion. Benali Saad, El Hassani Moulay El Mehdi, and Kouach Jaouad treated the patient, gathered the patient's clinical information, and supervised the project. All authors have read and approved the final version of the manuscript.
Table 1: CARE timeline - clinical course of Mrs. H.H., 65-year-old postmenopausal patient, HMI Mohamed V, Rabat, Morocco, November 2023
Figure 1: sagittal T2-weighted MRI sequences (six frames) of the pelvis
Figure 2: axial T2-weighted MRI sequences (four frames, upper pelvic cuts) of the pelvis
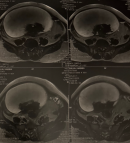
Figure 3: axial T2-weighted MRI sequences (six frames, lower pelvic cuts) of the pelvis
Figure 4: official MRI report (IRM pelvienne)
- Pan HT, Tu MQ, Zhang Y. Standardised management recommendations for uterine torsion: a systematic analysis of 96 cases. J Obstet Gynaecol Res. 2017;43(3):463-474.
- Muram D, Drouin P, Thompson DW. Incomplete uterine torsion: clinical and anatomical considerations. Am J Obstet Gynecol. 1982;142(8):1024-1028.
- Stewart EA. Uterine fibroids. Lancet. 2001;357(9252):293-298.
- Vollenhoven BJ, Lawrence AS, Healy DL. Uterine fibroids: a clinical review. Br J Obstet Gynaecol. 1990 Apr;97(4):285-98. PubMed | Google Scholar
- Murase E, Siegelman ES, Outwater EK, Perez-Jaffe LA, Tureck RW. Uterine leiomyomas: histopathologic features, MR imaging findings, differential diagnosis, and treatment. Radiographics. 1999 Sep-Oct;19(5):1179-97. PubMed | Google Scholar
- Dixit A, Bhatt S, Bhargava SK. Uterine torsion in a non-pregnant postmenopausal woman: a case report and literature review. J Clin Diagn Res. 2013;7(6):1211-1213.
- Miralles C, Orea M, España P, Provencio M, Sànchez A. Cancer antigen 125 associated with multiple benign and malignant pathologies. Ann Surg Oncol. 2003 Mar;10(2):150-4. PubMed | Google Scholar
- Baumgarten DA, Beall ME, Gomes AS. Uterine torsion: a cause of acute pelvic pain. Radiology. 1995;196(3):709-712.
- Mbatani N, Olawaiye AB, Prat J. Uterine sarcomas. Int J Gynaecol Obstet. 2018 Oct;143 Suppl 2:51-58. PubMed
- Sato K, Yuasa N, Fujita M, Fukushima Y. Clinical application of diffusion-weighted imaging for preoperative differentiation between uterine leiomyoma and leiomyosarcoma. Am J Obstet Gynecol. 2014 Apr;210(4):368.e1-368.e8. PubMed | Google Scholar
Search

This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures



Article metrics
Recently from the PAMJ-CM






