Spontaneous splenic rupture as a severe complication in a patient with chronic myeloid leukemia: a case report
Mohamed Zioui, Fatima Zahra Lahlimi, Illias Tazi
Corresponding author: Mohamed Zioui, Department of Clinical Hematology and Bone Marrow Transplantation, Mohammed VI University Hospital, Faculty of Medicine and Pharmacy, Cadi Ayyad University, Marrakesh, Morocco 
Received: 08 Dec 2023 - Accepted: 06 Jan 2024 - Published: 22 Mar 2024
Domain: Haematology,Oncology,General surgery
Keywords: Spontaneous rupture of the spleen, chronic myeloid leukemia, splenectomy, emergency
©Mohamed Zioui et al. PAMJ - Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Mohamed Zioui et al. Spontaneous splenic rupture as a severe complication in a patient with chronic myeloid leukemia: a case report. PAMJ - Clinical Medicine. 2024;14:31. [doi: 10.11604/pamj-cm.2024.14.31.42362]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com/content/article/14/31/full
Case report 

Spontaneous splenic rupture as a severe complication in a patient with chronic myeloid leukemia: a case report
Spontaneous splenic rupture as a severe complication in a patient with chronic myeloid leukemia: a case report
![]() Mohamed Zioui1,&,
Mohamed Zioui1,&, ![]() Fatima Zahra Lahlimi1,
Fatima Zahra Lahlimi1, ![]() Illias Tazi1
Illias Tazi1
&Corresponding author
Spontaneous splenic rupture is a rare and dreadful complication that can be life-threatening. Its association with hematological malignancies, including chronic myeloid leukemia, is very rare. CT scan is the reference radiological examination to confirm the diagnosis of spontaneous rupture of the spleen. Splenectomy is still a radical treatment. We report a case of a 35-year-old man followed for chronic myeloid leukemia with splenomegaly complicated by an acute and spontaneous rupture of the spleen revealed by intense abdominal pain, confirmed by CT scan. This case report illustrates a rare and critical entity of atraumatic splenic rupture in the presence of acute abdominal pain, particularly in patients with haematological malignancies. Accurate clinical diagnosis, abdominal CT scan, and prompt therapeutic intervention can improve the prognosis of patients already compromised by neoplasia.

Spleen rupture, a life-threatening situation, is often due to abdominal or thoracic trauma [1]. Spontaneous or atraumatic splenic rupture is a very rare complication [2]. Spontaneous splenic rupture (SSR) was first described in the 19th century [3]. In the majority of cases, SSR is caused by hematological malignancies (30.3%), infectious diseases (27.3%), and neoplastic diseases (20.0%). Other causes are drug-induced (9.2%) or mechanical disorders (6.8%) [4]. However, the association of SSR with chronic myeloid leukemia (CML) is very rare (0.72%) [5]. Splenectomy is the radical treatment for spontaneous splenic rupture [6]. We report a rare case of SSR as an acute complication of CML in a young man, requiring immediate diagnostic and therapeutic management to avoid hypovolemic shock.

Patient information: a 35-year-old patient, a former chronic smoker and previously treated for pulmonary tuberculosis. Referred to us for management of hyperleukocytosis found during investigation of persistent dyspnea.
Clinical findings: he was admitted conscious, apyretic, respiratory, and hemodynamically unstable, with oxygen saturation in arterial blood by pulse oximetry (SaO2) of 92% in room air. Clinical examination found a distended abdomen with splenomegaly and signs of right heart failure: jugular vein turgor, painful hepatomegaly, and leg oedema.
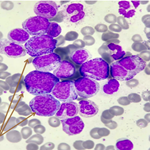
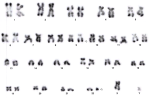
Diagnostic assessment: the blood count showed hyperleukocytosis (leukocytes: 508 000/mm3, neutrophils: 259 080/mm3, lymphocytes: 1 016/mm3 with the presence of a myeloma: metamyelocytes: 111 760/mm3, myelocytes: 76 200/mm3 and promyelocytes: 50 800/mm3), thrombocytosis: 882 000/mm3 and hemoglobin level: 11.7g/dl. Bone marrow aspiration showed an appearance in favor of CML with an estimated 3% marrow blast count. Karyotype confirmed the presence of the translocation t(9;22) (Figure 1). A chest X-ray revealed cardiomegaly with bilateral interstitial syndrome. Abdominal CT scan showed homogeneous hepatosplenomegaly with dilatation of the suprahepatic veins and inferior vena cava.
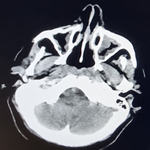
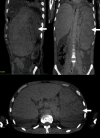
Timeline of the current episode: he then presented with acute, severe abdominal pain with a CT-scan appearance consistent with SSR over heterogeneous splenomegaly with foci of infarction and extensive hemoperitoneum (Figure 2).
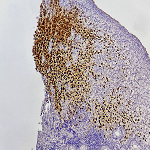
Therapeutic interventions: the patient was operated on for open splenectomy due to worsening hemodynamic status. Pathological examination of the splenectomy specimen revealed large necrotic foci with some atypical cells. Immunohistochemistry showed subacute inflammatory and necrotic changes with no underlying tumor proliferation.
Follow-up and outcome of interventions: the post-operative course was straightforward, the abdominal pain subsided, and the patient was put on an antiplatelet therapy based on low molecular weight heparin. The diagnosis of CML was retained, and the patient was put on Imatinib 400 mg/day with favorable follow-up and good clinical and biological outcome leading to hematological remission.
Patient perspective: during treatment, the patient was satisfied with the level of care provided to him.
Informed consent: the consent was obtained from the patient so that we could use the information for this case report.
Spontaneous splenic rupture or SSR in hematological malignancies is rare. Hodgkin's lymphoma and CML are the most frequently implicated [7]. Spontaneous splenic rupture can reach a mortality rate of up to 21% in the case of neoplastic diseases [8]. The physiophatology of SSR in hematological disorders is still unclear. In CML, SSR can be caused by infiltration of splenic parenchyma by tumor cells, leading to excessive spleen overload beyond the spleen's capacity to compensate and expand [9]. In addition, concomitant coagulation abnormalities may be responsible for subscapular hemorrhage and splenic infarction [5]. In our patient, leukemic infiltration and infarction are likely to be at the origin of the splenic rupture. However, our patient's hemostatic test was normal.
Diagnosis of SSR is very delicate. Patients present with acute abdominal pain, the most frequent symptom (95%) in patients with hematological malignancies, typically radiating to the left shoulder, combined with fever, nausea or emesis [4,5]. Abdominal ultrasound and CT scans, with a sensitivity and specificity of at least 95% in detecting splenic lesions, contribute to the diagnosis of splenic rupture and help rule out other causes of acute abdomen [5]. It often shows splenomegaly with splenic lacerations and intraperitoneal or subcapsular bleeding, as in our case [10]. Spontaneous splenic rupture (SSR) can be treated either surgically (splenectomy) or conservatively (clinical monitoring) [1]. Splenic artery embolization can be a safe and rapid procedure for patients for whom conservative management is planned [5]. However, the idea of performing a total splenectomy, the treatment option chosen in our case, may be justified due to tumor infiltration of the splenic parenchyma which may have already affected splenic function, resulting in functional hyposplenism [9].
This case report illustrates a rare and critical entity. Every physician should be alert to the possibility of atraumatic splenic rupture in the presence of acute abdominal pain, particularly in patients with haematological malignancies. Accurate clinical diagnosis, abdominal CT scan and prompt therapeutic intervention can improve the prognosis of patients already compromised by neoplasia.
The authors declare no competing interests.
Patient management: Mohamed Zioui, Fatima Zahra Lahlimi and Illias Tazi. Manuscript drafting: Mohamed Zioui and Fatima Zahra Lahlimi. Manuscript revision: Illias Tazi. All the authors have read and approved the final version of the manuscript.
We thank Dr Abakarim Ouadii for his contribution to this work and all the clinical staff who participated in treating the patient.
Figure 1: karyotype with t(9,22)
Figure 2: abdominal CT scan of splenic rupture
- Weaver H, Kumar V, Spencer K, Maatouk M, Malik S. Spontaneous splenic rupture: A rare life-threatening condition; diagnosed early and managed successfully. Am J Case Rep. 2013;14:13-5. PubMed | Google Scholar
- Kim HJ, Lee GW, Park DJ, Lee JD, Chang SH. Spontaneous Splenic Rupture in a Hemodialysis Patient. Yonsei Med J. 2005 Jun;46(3):435-438. PubMed | Google Scholar
- Miranda HV, Zarazúa ROM, Ramírez MAH, Briseño JAR, Maldonado GEM. Spontaneous splenic rupture in a patient with chronic granulocytic leukemia. Int Surg J. 2021;8:2786-8. PubMed | Google Scholar
- Kaniappan K, Lim CTS, Chin PW. Non-traumatic splenic rupture - a rare first presentation of diffuse large B-cell lymphoma and a review of the literature. BMC Cancer. 2018 Aug 2;18(1):779. PubMed | Google Scholar
- Jafferbhoy S, Chantry A, Atkey N, Turner D, Wyld L. Spontaneous splenic rupture: an unusual presentation of CML. BMJ Case Rep. 2011 Mar 24;2011:bcr0220113879. PubMed | Google Scholar
- Abbadi SE, Rhouni FZ, Jroundi L. Spontaneous splenic rupture: about a case and review of the literature. Pan Afr Med J. 2017 May 29;27:62. PubMed | Google Scholar
- Vemulakonda SHP, S SS, Jain A, Reddy A, Nelamangala Ramakrishnaiah VP. A Rare Case of Spontaneous Splenic Rupture as the Index Presentation of Chronic Myeloid Leukemia. Cureus. 2021 Nov 16;13(11):e19647. PubMed | Google Scholar
- Frost E, Patel A, Brill A. Atraumatic splenic rupture as an initial presentation of chronic myelogenous leukemia. J Community Support Oncol. 2017 Mar 1;15:113-5. Google Scholar
- Bauer TW, Haskins GE, Armitage JO. Splenic rupture in patients with hematologic malignancies. Cancer. 1981 Dec 15;48(12):2729-33. PubMed | Google Scholar
- Foreman BH, Mackler L, Malloy ED. Clinical inquiries. Can we prevent splenic rupture for patients with infectious mononucleosis. J Fam Pract. 2005 Jun;54(6):547-8. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures
Article metrics
Recently from the PAMJ-CM