
Primary cutaneous aspergillosis in a patient with idiopathic aplastic anemia: a case report
Mariem Ben Ticha, Yosra Soua, Nihed Abdessayed, Imen Khammeri, Asma Achour, Béchir Achour, Akila Fathallah, Yosra Ben Youssef, Wissem Hachfi
Corresponding author: Mariem Ben Ticha, Department of Infectious Diseases, Faculty of Medicine of Sousse, Farhat Hached University Hospital, Sousse, Tunisia 
Received: 10 Apr 2026 - Accepted: 22 Apr 2026 - Published: 12 Jun 2026
Domain: Dermatology,Infectious disease
Keywords: Case report, immunocompromised host, neutropenia, opportunistic infections, skin diseases
Funding: This work received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
©Mariem Ben Ticha et al. PAMJ Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Mariem Ben Ticha et al. Primary cutaneous aspergillosis in a patient with idiopathic aplastic anemia: a case report. PAMJ Clinical Medicine. 2026;21:10. [doi: 10.11604/pamj-cm.2026.21.10.52649]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com//content/article/21/10/full
Case report 

Primary cutaneous aspergillosis in a patient with idiopathic aplastic anemia: a case report
Primary cutaneous aspergillosis in a patient with idiopathic aplastic anemia: a case report
![]() Mariem Ben Ticha1,2,&,
Mariem Ben Ticha1,2,&, ![]() Yosra Soua3,4, Nihed Abdessayed1,5, Imen Khammeri6, Asma Achour3,7, Béchir Achour1,8,
Yosra Soua3,4, Nihed Abdessayed1,5, Imen Khammeri6, Asma Achour3,7, Béchir Achour1,8, ![]() Akila Fathallah1,6, Yosra Ben Youssef1,8, Wissem Hachfi1,2
Akila Fathallah1,6, Yosra Ben Youssef1,8, Wissem Hachfi1,2
&Corresponding author
Primary cutaneous aspergillosis is a rare invasive fungal infection occurring mainly in immunocompromised patients. This case highlights diagnostic challenges and emphasizes the importance of early mycological investigation. A 23-year-old man with severe idiopathic aplastic anemia presented with febrile neutropenia and a rapidly progressive painful necrotic skin lesion of the leg. Initial diagnosis suspected ecthyma gangrenosum. Histopathology revealed septate hyphae with acute angle branching. Culture identified Aspergillus flavus. Serum galactomannan was positive. Imaging showed no dissemination. The patient underwent surgical excision and received voriconazole. Local improvement was noted, but the patient died from bacterial septic shock. Necrotic skin lesions in immunocompromised patients unresponsive to antibiotics should prompt early biopsy and antifungal treatment.

Aspergillus spp. is the second most common cause of opportunistic fungal infection in humans after Candida [1,2]. This infection is often localized in the lungs, central nervous system (CNS), paranasal sinuses [3]. Cutaneous aspergillosis, both primary (PCA) and secondary (SCA), due to hematogenous dissemination of Aspergillus spp. is a relatively rare but life-threatening clinical manifestation and affects mostly immunocompromised patients [3]. Here we present a clinical case of an isolated PCA in a 23-year-old man with idiopathic aplastic anemia.

Patient information: a 23-year-old man with severe idiopathic aplastic anemia diagnosed in February 2019. He was treated with cyclosporine and transfusions. No relevant family or psychosocial history was reported.
Clinical findings: on admission, the patient presented with febrile neutropenia (temperature 39°C, absolute neutrophil count: 20/mm3) associated with chills and altered general condition. Cutaneous examination revealed a single circular erythematous and violaceous lesion located on the lateral aspect of the leg, with a central necrotic area (Figure 1). The lesion was painful, rapidly progressive, and initially described by the patient as a pustule. No other skin lesions were observed. There were no clinical signs suggestive of systemic involvement, particularly no pulmonary, neurological, or mucosal abnormalities.
Timeline: the patient was diagnosed with severe idiopathic aplastic anemia in February 2019 and started on immunosuppressive therapy with ciclosporin along with transfusion support. Two weeks later, he developed febrile neutropenia and was admitted to the hospital. At the same time, a skin lesion appeared on the leg and rapidly progressed to necrosis over a period of 10 days despite empirical broad-spectrum antibiotic therapy. A skin biopsy was performed, leading to the diagnosis of primary cutaneous aspergillosis. Surgical excision of the lesion was carried out, followed by initiation of antifungal therapy with voriconazole. Although local improvement was observed, the patient subsequently developed bacterial septic shock and died.
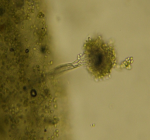
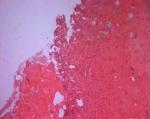
Diagnostic assessment: initial clinical suspicion was ecthyma gangrenosum; however, microbiological investigations were negative. Blood and urine cultures remained sterile, with no evidence of systemic bacterial infection. Mycological culture on Sabouraud dextrose agar showed characteristic macroscopic features with dark reverse pigmentation (Figure 2). Microscopic examination using the lamina technique confirmed the identification of Aspergillus flavus. Histopathological examination of the skin biopsy revealed abundant necrotic tissue containing numerous fungal elements (Figure 3A). Grocott staining demonstrated septate hyphae with acute-angle branching, highly suggestive of Aspergillus species (Figure 3B). Serum galactomannan antigenemia was positive, supporting the diagnosis of invasive aspergillosis. Cranial and whole-body computed tomography scans showed no evidence of pulmonary or systemic dissemination. The main differential diagnoses included ecthyma gangrenosum, bacterial skin infection, and pyoderma gangrenosum. Based on clinical, histopathological, and mycological findings, the final diagnosis of primary cutaneous aspergillosis was established. The prognosis was considered poor due to profound neutropenia and the underlying aplastic anemia.
Therapeutic intervention: the patient initially received empirical intravenous antibiotic therapy with piperacillin-tazobactam and vancomycin for seven days, which was later escalated to imipenem and ciprofloxacin due to lack of clinical improvement. Following diagnostic confirmation, surgical resection of the necrotic lesion was performed (Figure 4). Antifungal therapy with voriconazole (200 mg twice daily) was initiated. The modification of treatment was justified by the absence of response to antibacterial therapy and confirmation of fungal infection.
Follow-up and outcomes: after initiation of voriconazole and surgical management, local clinical improvement was observed with no further extension of the lesion. The antifungal treatment was well tolerated without reported adverse effects. No evidence of fungal dissemination was detected during follow-up. However, the patient subsequently developed bacterial septic shock and died, despite appropriate management, without evidence of secondary invasive aspergillosis.
Informed consent: it could not be obtained as the patient was deceased and no next of kin could be contacted. Patient anonymity has been strictly preserved in accordance with the Declaration of Helsinki.
Cutaneous invasive aspergillosis (CIA) is classified into primary and secondary forms. Primary cutaneous aspergillosis (PCA) results from direct inoculation of the fungus into the skin generally associated with a lesion or local injury, and the second from the blood spreading of hyphae where the lung is usually the portal of entry, from which the pathogen may disseminate to almost any organ, often the brain and skin [1,4]. Primary cutaneous aspergillosis (PCA) is rare; few case reports and series have been published [1]. Cases have been described in neonates, in HIV/AIDS patients, cancer, especially hematological diseases, solid organ transplantation, etc. [1,3]. Primary cutaneous aspergillosis (PCA) may manifest with a nodule, pustule, papule, erythematous plaque, which may progress to central necrosis, or hemorrhagic bullae [5,6]. The microorganisms most often involved are Aspergillus flavus and Aspergillus fumigatus [1,7].
Several conditions can be confused with a CIA, such as pyoderma gangrenosum, ecthyma gangrenosum, malignant or inflammatory dermatoses [8]. Diagnosis relies on histopathological identification of septate hyphae with acute-angle branching and confirmation by fungal culture [1]. Although serum galactomannan may support the diagnosis of invasive aspergillosis, it does not reliably distinguish between primary and secondary cutaneous forms [7]. Cranial computed tomography scan, fundus examination of the eyes, whole body computed tomography scan, and lumbar puncture are important to rule out an secondary cutaneous aspergillosis (SCA) [1]. Combined surgical debridement and systemic antifungal therapy-particularly voriconazole, which is recommended as first-line therapy-are associated with improved outcomes [7,9]. Prognosis depends largely on immune status, degree of neutropenia, and early initiation of antifungal therapy [1]. In our case, despite appropriate antifungal treatment and local improvement, the patient died after developing septic shock following a bacterial infection with a multidrug-resistant organism.
Primary cutaneous aspergillosis should be suspected in immunocompromised patients presenting with necrotic skin lesions unresponsive to antibacterial therapy. Early biopsy and mycological investigation are crucial to establish the diagnosis and initiate prompt antifungal treatment, which may improve prognosis.
The authors declare no competing interests.
All the authors have read and approved the final version of this manuscript.
Figure 1: erythematous-violaceous skin lesion with central necrosis
Figure 2: macroscopic appearance of Aspergillus flavus culture on Sabouraud agar
Figure 3: A) histopathological examination showing necrotic tissue with fungal elements (H&E, x100); B) grocott staining showing septate hyphae with acute-angle branching (x100)
Figure 4: skin lesion after surgical excision
- Torrelo A, Hernández-Martín A, Scaglione C, Madero L, Colmenero I, Zambrano A. Primary cutaneous aspergillosis in a leukemic child. Actas Dermosifiliogr. 2007;98(4):276-8. PubMed | Google Scholar
- Furlan KC, Pires MC, Kakizaki P, Chartuni JC, Valente NY. Primary cutaneous aspergillosis and idiopathic bone marrow aplasia. An Bras Dermatol. 2016;91(3):381-3. PubMed | Google Scholar
- Kishore M, Gupta P, Bhardwaj M. Cytomorphological diagnosis of isolated cutaneous aspergillosis in an immunocompetent host. Indian Dermatol Online J. 2018;9(3):206-8. PubMed | Google Scholar
- Muñoz P, Guinea J, Bouza E. Update on invasive aspergillosis: clinical and diagnosis aspects. Clinical Microbiology and infection. 2006;12(7):24-39. Google Scholar
- Tunçcan ÖG, Aki Z, Akyürek N, Sucak G, enol E. Isolated cutaneous aspergillosis in an acute lymphoblastic leukemia patient after allogeneic stem cell transplantation. J Infect Dev Ctries. 2011;5(5):406-9. PubMed | Google Scholar
- Camus M, Anyfantakis V, Dammak A, Riche A, Delouane H, Roblot F, Guillet G. Primary cutaneous aspergillosis in an immunocompetent farmworker. Ann Dermatol Venereol. 2010;137(5):373-6. PubMed | Google Scholar
- Bernardeschi C, Foulet F, Ingen-Housz-Oro S, Ortonne N, Sitbon K, Quereux G et al. Cutaneous invasive aspergillosis: retrospective multicenter study of the French invasive aspergillosis registry and literature review. Med (Baltimore). 2015;94(26):e1018. PubMed | Google Scholar
- Teagle A, Hargest R. Management of pyoderma gangrenosum. Journal of the Royal Society of Medicine. 2014;107(6):228-36. PubMed | Google Scholar
- Patterson TF, Thompson GR, Denning DW, Fishman JA, Hadley S, Herbrecht R et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis 2016 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2016;15;63(4):e1-e60. PubMed | Google Scholar
Search

This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures


Article metrics
Recently from the PAMJ-CM






