
Community perceptions and perceived causes of preeclampsia and eclampsia in Sidama region, Ethiopia: a qualitative study
Birhanu Jikamo, Mulat Adefris, Telake Azale, Kassahun Alemu
Corresponding author: Birhanu Jikamo, Hawassa University College of Medicine and Health Sciences, Hawassa, Southern Nations, Ethiopia 
Received: 18 Mar 2022 - Accepted: 04 Jun 2026 - Published: 15 Jun 2026
Domain: Obstetrics and gynecology,Community health,Maternal and child health
Keywords: Community, perception, pre-eclampsia, eclampsia, Ethiopia
Funding: This work received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
©Birhanu Jikamo et al. PAMJ Clinical Medicine (ISSN: 2707-2797). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Birhanu Jikamo et al. Community perceptions and perceived causes of preeclampsia and eclampsia in Sidama region, Ethiopia: a qualitative study. PAMJ Clinical Medicine. 2026;21:12. [doi: 10.11604/pamj-cm.2026.21.12.34315]
Available online at: https://www.clinical-medicine.panafrican-med-journal.com//content/article/21/12/full
Research 

Community perceptions and perceived causes of preeclampsia and eclampsia in Sidama region, Ethiopia: a qualitative study
Community perceptions and perceived causes of preeclampsia and eclampsia in Sidama region, Ethiopia: a qualitative study
![]() Birhanu Jikamo1,&, Mulat Adefris2, Telake Azale2,
Birhanu Jikamo1,&, Mulat Adefris2, Telake Azale2, ![]() Kassahun Alemu2
Kassahun Alemu2
&Corresponding author
Introduction: despite national declines in maternal mortality, preeclampsia remains a major public health concern in the Sidama Region of Ethiopia. Limited evidence exists on community perceptions of preeclampsia and eclampsia. Therefore, this study explored community perceptions and perceived causes of preeclampsia and/or eclampsia in the Sidama Region, southern Ethiopia.
Methods: a phenomenological study was conducted in communities of the Sidama Region from January to August 2021. Participants were selected purposively, and data were collected through face-to-face in-depth and key informant interviews conducted in the Sidamic language. Interviews explored perceptions of prevention, signs and symptoms, causes, and treatment of preeclampsia/eclampsia. All interviews were audio-recorded, transcribed, and analyzed using thematic coding. Differences in coding were discussed and resolved by the research team.
Results: the study found that community perceptions of preeclampsia and eclampsia in the Sidama Region differed greatly from biomedical explanations. Participants believed that stress, emotional problems, marital conflict, and eating salty foods cause preeclampsia, while cold exposure, cold drinks, supernatural forces, and fire exposure were seen as causes of eclampsia. Perceptions of prevention, symptoms, and treatment, including traditional and medical approaches, also differed considerably from current scientific evidence.
Conclusion: community perceptions of preeclampsia and eclampsia in the Sidama Region differed markedly from biomedical understanding, and awareness of these conditions was low. These findings emphasize the need for maternal and child health providers to address local beliefs and knowledge gaps through targeted health education, counseling, and maternal healthcare services.

Preeclampsia and eclampsia are among the leading causes of maternal morbidity and mortality worldwide and rank as the second most common causes in many countries [1]. Preeclampsia is characterized by new-onset hypertension (≥140/90 mmHg) occurring after 20 weeks of gestation in a previously normotensive woman, accompanied by proteinuria (≥1+ on dipstick testing or ≥0.3 g/L of urine protein), with blood pressure measurements taken on two occasions at least four hours apart [1]. eclampsia is defined as the occurrence of generalized tonic-clonic seizures in a woman with preeclampsia that cannot be attributed to other causes and occurs in the absence of pre-existing neurological disorders [1].
In sub-Saharan Africa, hypertensive disorders of pregnancy (HDPs) were the second leading cause of maternal mortality in 2021, following obstetric hemorrhage. Obstetric hemorrhage accounted for 28.8% of maternal deaths, while HDPs contributed to 22.1% [2]. Similarly, a study conducted in southern Ethiopia in 2019 identified HDPs as the third leading cause of maternal mortality, accounting for 16% of deaths, after obstetric hemorrhage (39%) and anemia (28%) [3]. The same study reported that severe preeclampsia (51.8%) and postpartum hemorrhage (24.9%) were the most common complications leading to hospital admission. Furthermore, eclampsia accounted for 70% of pregnancy-related complications that developed more than 12 hours after admission [3].
In low-income countries, the utilization of maternal health services is strongly influenced by cultural beliefs and values, which shape individuals´ perceptions of health, illness, and healthcare-seeking behavior [4]. This is particularly relevant in Ethiopia, where diverse cultural practices, limited awareness, delayed care-seeking, and misconceptions surrounding preeclampsia and eclampsia contribute to persistent maternal health challenges. Although nationally representative data on the prevalence of these conditions are lacking, preeclampsia and eclampsia remain major causes of maternal morbidity and mortality in Ethiopia [5]. Furthermore, existing studies from southern Ethiopia on community perceptions of preeclampsia and eclampsia are limited in scope, do not adequately explore community-level factors influencing their prevention and management, and often exclude women with a history of preeclampsia [5,6]. This version improves flow, avoids repetition, strengthens the academic tone, and clearly establishes the research gap.
In Ethiopia, the pooled prevalence of hypertensive disorders of pregnancy (HDPs) was estimated at 6.07% in 2018 [7]. Despite ongoing efforts to improve maternal healthcare, significant inequities persist in the utilization of maternal health services both between and within regions of the country [8]. Geographic variations in the burden of HDPs have also been reported. The lowest prevalence was observed in Addis Ababa (5.41%), whereas the Sidama Region had a substantially higher pooled prevalence of 10.13% [7]. These findings highlight marked regional disparities in the occurrence of HDPs and underscore the need for context-specific interventions to address maternal health challenges in high-burden areas [7,8].
Several factors have been identified as being associated with preeclampsia and eclampsia in Ethiopia, including women´s decision-making autonomy, previous obstetric complications, primigravidity, lack of formal education, low socioeconomic status, occupation as a housewife, timely healthcare-seeking behavior, and antenatal care (ANC) attendance [9-13]. In addition, women with greater knowledge of preeclampsia were more likely to have utilized ANC services, delivered in health facilities, and reported a history of previous obstetric complications [14]. These findings suggest that socioeconomic, reproductive, and healthcare-related factors play important roles in shaping both the risk of preeclampsia and eclampsia and women's awareness and utilization of maternal health services.
To date, most research on preeclampsia and eclampsia in the Sidama Region has focused on clinical and hospital-based evidence, with limited attention given to community perspectives [3,9-12,15]. This lack of community-based evidence has constrained efforts to develop effective strategies for the prevention, early detection, and management of preeclampsia and eclampsia in the region [15]. Previous studies have emphasized the importance of addressing individual- and community-level barriers through the engagement of community members and women with a history of preeclampsia [5]. Understanding community perceptions of preeclampsia and eclampsia is therefore essential for informing culturally appropriate interventions, policies, and health education programs aimed at improving maternal health outcomes. The findings of this study may assist maternal and child health providers in the Sidama Region to identify misconceptions and negative perceptions early in pregnancy and tailor educational and counseling efforts accordingly. Therefore, this study aimed to explore community perceptions of preeclampsia and eclampsia among communities in the Sidama Region of southern Ethiopia.

Study design and setting: a phenomenological study was conducted in communities of the Sidama region from January to August 2021. The 2020 population of the region was approximately 4 million, with 13 public hospitals, 138 health centers, and 540 health posts that provided maternal, newborn, and child health services. In 2020, approximately 132,031 pregnant women attended ≥4 antenatal care visits, and 127,585 women gave birth. We chose communities in the catchment area of seven public hospitals purposively.
Study population: the participants of this study included women who experienced preeclampsia or eclampsia during their most recent pregnancy, their husbands or partners, and traditional birth attendants from communities in the Sidama Region.
Sampling strategy: purposive sampling was employed to select study participants. Women who experienced preeclampsia or eclampsia during their most recent pregnancy were identified based on existing antenatal care records, in consultation with hospital administrators, community leaders, and health extension workers. Husbands or partners were invited to participate when they had accompanied their wives during the pregnancy affected by preeclampsia and/or eclampsia. Traditional birth attendants were selected through consultation with community leaders and health extension workers, with inclusion criteria being experience in assisting births within the community from home settings.
Data collection
Interview tool preparation: we prepared an interview tool to guide data collection. This was translated into the Sidamic local language and translated back to English for analysis. Note takers practiced and familiarized themselves with the questions before conducting the interviews, and had a background in maternity and reproductive health. The questionnaire included a section on socio-demographic characteristics and asked participants about their occupation, maternal age, marital status, place of residence, and level of education. Preeclampsia and eclampsia were defined, and participants were asked to give their perceived local names for the diseases. Additional information was collected by probing respondents for prevention strategies, signs and symptoms, perceived causes, and traditional and clinical treatments. A pilot test was conducted with seven eligible women to ensure the interview guide was clear and understandable. Interviews were held in homes, hospitals, and workplaces. We did not carry out repeat interviews with the same participants. The interviewer had no relationship with the participants before the beginning of this study.
In-depth interviews: we conducted face-to-face in-depth interviews (IDIs) with female participants for approximately 45-60 minutes. The principal investigator and two note-takers gathered data. We audio-recorded all the interviews. We asked open-ended questions at the beginning of an interview to identify themes.
Key informant interviews: we conducted face-to-face key informant interviews with husbands/partners and traditional birth attendants. We recorded all interviews. There was no set time limit for the interviews, as a conducive environment was set for participants´ free exchange of ideas and detailed responses. Data were collected by principal investigators and two note-takers for consistency of information.
Data analysis
In-depth interviews analysis: the audio transcript was processed into a MS Word document. The study researchers listened to and read the transcripts to thoroughly understand the content and meaning. We used Open Code software to identify relationships between the aim of the research and findings from raw data. We categorized participants' responses by using an inductive coding thematic approach to identify themes. Data coding continued until saturation was reached, and no new concepts emerged from the data. The completed code structure was applied to develop and report themes, and consensus was reached among the researchers. A thematic chart was created from the identified themes in the coding. Verbatim quotations from the transcripts were used to present the results of the respondents. Any differences in thematic coding were resolved by discussion among team members.
Key informant interviews analysis: analysis of the data was conducted based on the audio recordings of the interviews and/or audio transcriptions. The research team transcribed the records of the interview and translated them into English suitability for analysis. The transcripts were read and re-read by the corresponding author to ensure they were complete. All the audios were listened to by two co-authors (KA and MA) to check that they corresponded with the transcriptions. Thematic content analysis with an inductive, data-driven approach was used to transcribe interview texts. The study researchers read the transcripts to understand the content and meaning. Three researchers performed the coding process, and any differences in thematic coding were resolved by discussion among team members. The trustworthiness of the coding was ensured by giving the transcription to the first five participants to check if the transcription truly reflected their perceptions. The trustworthiness of the coding was also ensured by including: self-reflectivity, member check, thick description of the content, and a detailed description of the methodology.
Ethical considerations: ethical approval was obtained from the Institutional Review Board of the University of Gondar (Ref. No. O/V/P/RCS/044/2019) in March 2019. Additional ethical clearance and permission were granted by the Ethical Review Committee of the Sidama Regional Health Bureau Research and Technology Transfer Office. Authorization to conduct the study was secured from relevant administrative authorities at all levels. Participants were informed about the study objectives and procedures before data collection, and verbal informed consent, including consent for audio recording, was obtained from all participants.
Socio-demographic characteristics of study participants we conducted in-depth interviews with 39 women who had experienced preeclampsia and/or eclampsia in the most recent pregnancy. Key informant interviews were conducted with 13 husbands or partners and five traditional birth attendants. After 57 interviews, we confirmed that no new information was generated and that data saturation was reached. Eighteen of the women (40.91%) were 25-34 years old, and six (46.15%) of the male participants were ≥35 years old. The mean age of the women was 22.10(±2.24) years old, and their husbands/partners were 24.45(SD: ±4.83) years old. The majority, 40(90.90%) of the women were married. Sixteen of the women (36.36%) who did not attend school and 32 (72.72%) resided in rural areas (Table 1).
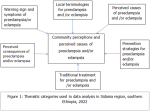
Identified themes from in-depth and key informant interviews: six themes were identified from our analysis by reviewing different literature: 'local terminologies', 'perceived causes and traditional treatments/managing conditions', 'prevention strategies', 'perceived consequences', and 'warning signs and symptoms of preeclampsia and/or eclampsia' (Figure 1).
Theme 1: local terminologies for preeclampsia and/or eclampsia
There were no local terms for preeclampsia and/or eclampsia in the study area. Preeclampsia and/or 'eclampsia' were not well-known terms or conditions in the study communities of the Sidama region.
Theme 2: perceived causes and traditional treatment for preeclampsia and/or eclampsia
Local beliefs concerning the causes of preeclampsia and/or eclampsia were not associated with those of scientific/research findings. Participants´ stated perceived causes for preeclampsia were identified as stress, depression, tension, conflict with the husband, and eating food with a high salt content, whereas, for eclampsia, perceived causes were identified as sleeping on a cold floor, drinking cold liquids, supernatural forces and evil eyes, and exposure to fire during pregnancy. There was no identified traditional treatment for preeclampsia in the study area. For eclampsia, respondents mentioned traditional treatments such as the smell of onion, herbal or self-treatments, and belief in holy water were used to treat convulsions before accessing care in health institutions. These findings were supported by one of the participants [married, 34 years old, rural]. "The smell of onion was considered a traditional treatment for eclampsia.” This idea was supported by one of the study participants [husband, 35 years old, rural]. “Herbal remedies or self-treatment were also reported as traditional approaches for managing eclampsia." This finding was said by one of the study participants [married, 25 years old, urban]. “Beliefs in holy water were noted as a traditional treatment for eclampsia.”
The present results narrated by one of the participants [married, 27 years old, rural]. “Participants reported having limited knowledge about the maternal complications associated with preeclampsia and/or eclampsia during convulsive episodes. Many perceived the condition as caused by the evil eye or supernatural forces and sought help by visiting spiritual houses for prayers.” More than ten percent of participants (6; 10.5%) reported that depression during pregnancy could cause preeclampsia, while 8% (5; 8.8%) attributed it to stress during pregnancy. Regarding eclampsia, 5 participants (8.8%) believed it could be caused by sleeping on a cold floor, and 6 participants (10.5%) cited drinking cold liquids during pregnancy as a cause. These perceptions were illustrated by one participant [husband, 34 years old, rural], who stated: “Pregnant women who eat food with a high salt content get preeclampsia.”
These perceptions were illustrated by one participant [married, 17 years old, urban], who stated: “Drinking cold liquids during pregnancy can cause eclampsia.” These perceptions were highlighted by one participant [married, 33 years old, rural], who stated: “Supernatural forces and evil eyes are the cause of eclampsia and further affect women during pregnancy, delivery, and newborns after birth.” (Table 2)
Theme 3: prevention strategies for preeclampsia and/or eclampsia
Local beliefs concerning the early prevention of preeclampsia and/or eclampsia were not associated with scientific/research findings. Participants identified several perceived strategies for preventing preeclampsia, including financial support, restriction of dietary salt intake, provision of psychological and emotional support, and increased consumption of fruits and vegetables. For eclampsia, prevention strategies were largely linked to spiritual beliefs. These perceptions were illustrated by one participant [married, 21 years old, rural], who stated: “Eating fruits and vegetables during pregnancy can reduce the occurrence of preeclampsia and/or eclampsia.”
These perceptions were further illustrated by one participant [married, 26 years old, urban], who stated: “Financial support during pregnancy can reduce preeclampsia and/or eclampsia, and financial barriers affect access to transportation, availability of medicine, and affordability of services.” Participants emphasized the role of dietary practices in preventing preeclampsia and eclampsia. One participant [husband, 32 years old, rural] explained: “Participants also stated that pregnant women who engaged in perceived healthy dietary habits, including salt restriction, while reducing perceived unhealthy dietary habits, which are important for both the mother and the proper growth of the fetus.”
Theme 4: perceived consequences of preeclampsia and/or eclampsia
Participants reported that the consequences of preeclampsia and/or eclampsia included abortion, cesarean delivery, and maternal death. These perceptions were illustrated by one participant [married, 27 years old, rural] who stated: “Women who have preeclampsia or eclampsia during pregnancy can end up with maternal death.” The current findings were illustrated by one participant [husband, 37 years old, urban], who stated: “An abortion during pregnancy can be a consequence of preeclampsia and/or eclampsia.” The finding was illustrated by one participant [married, 22 years old, urban], who stated: “Cesarean delivery during pregnancy can be an outcome of preeclampsia and/or eclampsia.”
Theme 5: warning signs and symptoms of preeclampsia/or eclampsia
We found that the community had limited knowledge regarding the signs and symptoms of preeclampsia and/or eclampsia. Participants identified several warning signs, including swollen feet, weakness during pregnancy, sweating, and headaches. These perceptions were illustrated by one participant [married, 29 years old, rural], who stated: “Having swollen feet during pregnancy could be a warning sign of preeclampsia and/or eclampsia.” These findings were reported by one of the participants [husband, 37 years old, rural]: "Feeling weak during pregnancy could be a warning sign of preeclampsia and/or eclampsia." These findings were reported by one of the participants [married, 23 years old, urban]: "Sweating during pregnancy could be a warning sign of preeclampsia and/or eclampsia."
This study aimed to explore community perceptions and perceived causes of preeclampsia and/or eclampsia in the Sidama region, southern Ethiopia. We found that community perceptions of preeclampsia and/or eclampsia in the Sidama region differed substantially from established biomedical explanations. There were no local terms for preeclampsia and/or eclampsia, and community knowledge of their signs and symptoms was limited. Participants commonly attributed the conditions to psychosocial stressors (such as stress, depression, tension during pregnancy, and marital conflict) and dietary factors, particularly high salt intake. Perceived causes of eclampsia included sleeping on a cold floor, drinking cold liquids, exposure to fire, and supernatural influences such as evil spirits or the evil eye. Our findings indicate that community perceptions of preeclampsia and/or eclampsia in the Sidama region diverge from biomedical explanations. This may reflect limited and non-repetitive antenatal health education, which is insufficient to ensure a comprehensive understanding of the clinical causes [16]. Additionally, variations in women´s educational levels and access to health information likely contribute to these misconceptions. These results highlight the need to strengthen and redesign antenatal health education programs to emphasize the biomedical causes of preeclampsia and eclampsia, thereby improving community awareness, early recognition of danger signs, and timely maternal health care utilization [16].
The absence of local terms for preeclampsia and/or eclampsia in the study areas aligns with previous findings that these conditions are poorly recognized as pregnancy-related diseases and lack culturally specific nomenclature [17-19]. Recognition and timely detection of preeclampsia are influenced by women´s knowledge, personal experiences, cultural beliefs, and social context [20], with studies reporting that up to 50% of pregnant women misidentify hypertensive disorders of pregnancy [21]. These findings underscore the importance of community-based education to raise awareness of pregnancy danger signs, promote early recognition of severe obstetric complications, and improve maternal health care utilization [9].
Herbal remedies were commonly reported as traditional treatments for eclampsia, reflecting limited knowledge of preeclampsia and eclampsia and potentially delaying early recognition of danger signs [21]. Consistent with previous studies, community attitudes and behaviors toward maternal health care utilization influenced care-seeking practices [22], with urban-rural disparities further affecting access to services. These findings highlight the need for community mobilization and targeted awareness campaigns to correct misconceptions and promote timely use of maternal health care services.
Community knowledge of the signs and symptoms of preeclampsia and/or eclampsia in the Sidama region was limited, with 22.7% of pregnant women reportedly unaware of the causes of newborn deaths [23]. In contrast, other studies have shown higher levels of awareness, with 50.4% of participants recognizing at least three danger signs of preeclampsia/eclampsia [24] and 38.9% identifying at least one sign of pregnancy-induced hypertension [5]. These discrepancies may reflect differences in awareness, educational attainment, and socioeconomic status, which are important determinants of timely health-seeking behavior and maternal outcomes.
Stress was commonly perceived as a cause of preeclampsia, aligning with evidence that psychological stress during pregnancy is associated with elevated blood pressure and increased risk of preeclampsia [19,20,25]. Regular antenatal care visits offer opportunities to screen high-risk women and implement early interventions to mitigate adverse pregnancy outcomes [21]. Community health extension workers, supported by pregnancy registries and family folders, play a vital role in promoting ANC attendance and enhancing the delivery of maternal health services.
Depression during pregnancy was perceived as a cause of preeclampsia, consistent with evidence linking depressive symptoms and sleep disturbances to hypertension and an increased risk of preeclampsia/eclampsia [26,27]. Antenatal care visits provide a key platform for delivering health education on pregnancy-related conditions and promoting maternal and child health [16]. Additionally, maternal health care utilization is shaped by socioeconomic factors such as wealth, employment, and decision-making autonomy, which are important determinants of timely care-seeking [28].
Participants perceived tension during pregnancy as a cause of preeclampsia, consistent with studies linking excessive worry and stress-arising from financial concerns, birth preparation, and fear of complications-to hypertension during pregnancy [25,29]. Such stressors may contribute to adverse maternal and perinatal outcomes. Variations in ANC attendance and the methods used to deliver antenatal health education may affect community understanding of these conditions, highlighting the need for improved awareness strategies. Participants perceived conflict with the husband as a cause of preeclampsia, consistent with evidence linking spousal mistreatment to increased stress and elevated risk of hypertension during pregnancy [14,26]. Furthermore, a husband´s financial support has been identified as a key determinant of maternal health care utilization, with a lack of support limiting women´s ability to make decisions regarding their health needs [30].
Participants perceived sleeping on a cold floor as a cause of eclampsia, which contrasts with clinical evidence identifying abnormal placentation, vascular disturbances, oxidative stress, and endothelial damage as the primary causes of preeclampsia/eclampsia [1,3,23]. This discrepancy likely reflects limited community awareness and underscores the importance of regular ANC visits, routine blood pressure and proteinuria monitoring, education on danger signs, and early identification of risk factors to improve understanding and timely management. Supernatural forces were perceived as a cause of eclampsia, consistent with studies showing that community beliefs often attribute the condition to spiritual causes [24,31]. For instance, 29.6% of participants reported managing eclampsia using a combination of hospital care and spiritual interventions [24]. Cultural norms, beliefs, and values strongly influence women´s health care-seeking behaviors [27]. Enhancing community-based awareness of the clinical causes of eclampsia may help correct these misconceptions and promote timely care.
Participants perceived salt restriction during pregnancy as a preventive measure for preeclampsia, consistent with evidence that reducing high salt intake can lower the risk of hypertension and preeclampsia [26]. Adequate nutrition, including a balanced diet, supports maternal health and may contribute to prevention [32]. Nevertheless, some participants reported inconsistent adherence to salt restriction despite awareness of its potential health risks [32], highlighting the need for reinforced dietary counseling during antenatal care. Consumption of fruits and vegetables was identified as a strategy to prevent preeclampsia, consistent with studies reporting that frequent ANC visits, adequate rest, and vegetable intake were recognized preventive measures by 78.1%, 50.2%, and 57.4% of participants, respectively [21]. Variations in adherence may be influenced by financial constraints, low literacy, community perceptions of preeclampsia/eclampsia, and limited access to or prior experiences with health facilities [28].
Some participants perceived spiritual practices as a preventive strategy for eclampsia, reflecting limited understanding of its clinical causes and reliance on traditional home remedies [26,33]. In contrast, other studies indicate that most participants recognize prevention through regular antenatal care (76.4%) and hospital delivery (70.8%) [24]. Overall knowledge of preeclampsia prevention and management among participants was reported as poor (22.5%), moderate (48.8%), and good (28.8%) [14], highlighting gaps in awareness that need to be addressed through targeted education.
No traditional treatments for preeclampsia were reported in the study area, consistent with previous findings [29]. This contrasts with studies indicating that cultural preferences for traditional medicine, mistrust of modern healthcare, and beliefs in the protective powers of traditional birth attendants may reduce prenatal care utilization [34,35]. Limited access to maternity services, low education, low income, and geographic barriers have also been identified as factors driving reliance on traditional remedies [35]. The use of onion aroma as a traditional treatment for eclampsia was reported, consistent with studies showing that home remedies are often used before seeking formal care [36,37].
Strengths and limitations of the study
Strength of our study was the use of qualitative methods, specifically in-depth interviews and key informant interviews, which provided rich insights into perceptions of preeclampsia and/or eclampsia. One limitation was that the perspectives of policymakers were not incorporated, and the geographical scope was limited; therefore, the findings may lack generalizability.
Community perceptions of preeclampsia and eclampsia in the Sidama region differed from biomedical explanations, and no local terms existed for these conditions. Participants perceived the causes of preeclampsia to include stress, depression, tension, spousal conflict, and high salt intake. In contrast, perceived causes of eclampsia included sleeping on a cold floor, drinking cold liquids, supernatural forces, and exposure to fire. These findings underscore the need for strengthened, repeated, and context-specific antenatal health education to improve awareness, correct misconceptions, and promote timely utilization of maternal health care services within the community.
What is known about this topic
- Most studies on preeclampsia and eclampsia in the Sidama region focus on clinical and hospital-based findings, with limited community-level evidence;
- Evidence on community perceptions of preeclampsia and eclampsia in southern Ethiopia is insufficient, particularly regarding women with a history of the condition;
- Previous research recommends further qualitative investigation to explore individual- and community-level barriers to preeclampsia management.
What this study adds
- Community perceptions of preeclampsia and eclampsia in the Sidama region differ from biomedical explanations;
- Preeclampsia was linked to stress, depression, tension, spousal conflict, and high salt intake; eclampsia to cold exposure and supernatural forces;
- No local terms existed for preeclampsia or eclampsia, and these conditions were not well recognized in the community.
The authors declare no competing interests.
This study was conducted collaboratively by all authors. Birhanu Jikamo, Mulat Adefris, and Kassahun Alemu contributed to conceptualization, study design, data curation, analysis, and drafting the manuscript. Birhanu Jikamo, Mulat Adefris, Telake Azale, and Kassahun Alemu managed the investigation, conducted literature searches, reviewed methodology, and collected data. All authors contributed to manuscript review, resource preparation, and editing. They have read and approved the final version of this manuscript.
We thank the University of Gondar, Institute of Public Health, College of Medicine and Health Sciences for providing us the opportunity to conduct this study. We also thank supervisors for reviewing and editing the report of this PhD project. We thank Dorothy L. Southern for her critical review of this paper and for her support in editing and training in scientific writing. We also thank the study participants who participated in this study.
Table 1: socio-demographic and economic characteristics of study participants in the Sidama region of southern Ethiopia, 2022
Table 2: perceived causes of preeclampsia and eclampsia in the community of Sidama region, southern Ethiopia, 2022
Figure 1: thematic categories used in data analysis in the Sidama region, southern Ethiopia, 2022
- Brown MA, Magee LA, Kenny LC, Karumanchi SA, McCarthy FP, Saito S et al. International Society for the Study of Hypertension in Pregnancy (ISSHP). Hypertensive Disorders of Pregnancy: ISSHP Classification, Diagnosis, and Management Recommendations for International Practice. Hypertension. 2018;72(1):24-43. PubMed | Google Scholar
- Musarandega R, Nyakura M, Machekano R, Pattison R, Munjanja SP. Causes of maternal mortality in Sub-Saharan Africa: A systematic review of studies published from 2015 to 2020. J Glob Health.2021;11:04048. PubMed | Google Scholar
- Wakgar N, Dulla D, Daka D. Maternal near misses and death in southern Ethiopia: a retrospective study. Ethiopian Journal of Reproductive Health. 2019 Apr 30;11(2):9. Google Scholar
- Beardmore-Gray A, Vousden N, Charantimath U, Katageri G, Bellad M, Kapembwa K et al. Planned early delivery versus expectant management to reduce adverse pregnancy outcomes in pre-eclampsia in a low- and middle-income setting: study protocol for a randomized controlled trial (CRADLE-4 trial). Trials. 2020;21(1): 960. PubMed | Google Scholar
- Sripad P, Ismail H, Dempsey A, Kirk K, Warren CE. Exploring barriers and opportunities for pre-eclampsia and eclampsia prevention and management in Ethiopia. Ending Eclampsia Report. Washington, DC: Population Council. 2018. Google Scholar
- Gudu W, Sripad P. Barriers to the Detection, Management and Prevention Of Preeclampsia/Eclampsia In Ethiopia. EJRH. 2020;12(4). Google Scholar
- Berhe AK, Kassa GM, Fekadu GA, Muche AA. Prevalence of hypertensive disorders of pregnancy in Ethiopia: a systemicreview and meta-analysis. BMC pregnancy and childbirth. 2018;181):34. PubMed | Google Scholar
- Abegaz KH, Mohammed AA. Healthcare expenditure and GDP in Ethiopia from 1995 to 2014: a time-series analysis. Agriculture & Food Security. 2018 Jul 13;7(1):47. PubMed | Google Scholar
- Tessema KF, Gebremeskel F, Getahun F, Chufamo N, Misker D. Individual and Obstetric Risk Factors of Preeclampsia among Singleton Pregnancy in Hospitals of Southern Ethiopia. Int J Hypertens. 2021 Jan 20:2021:7430827. PubMed | Google Scholar
- Seyom E, Abera M, Tesfaye M, Fentahun N. Maternal and fetal outcome of pregnancy related hypertension in Mettu Karl Referral Hospital, Ethiopia. J Ovarian Res. 2015 Mar 15:8:10. PubMed | Google Scholar
- Endeshaw G, Berhan Y. Perinatal Outcome in Women with Hypertensive Disorders of Pregnancy: A Retrospective Cohort Study. Int Sch Res Notices. 2015 Jan 8;2015:208043. PubMed | Google Scholar
- Berhan Y, Berhan A. Causes of maternal mortality in Ethiopia: a significant decline in abortion related death. Ethiop J Health Sci. 2014 Sep;24 Suppl(0 Suppl):15-28. PubMed | Google Scholar
- Ministry of Health Ethiopia. Health Sector Transformation Plan II. Ministry of Health Ethiopia. 2020/21-2024/25.
- Mekie M, Addisu D, Bezie M, Melkie A, Getaneh D, Bayih WA et al. Knowledge and attitude of pregnant women towards preeclampsia and its associated factors in South Gondar Zone, Northwest Ethiopia: a multi-center facility based cross-sectional study. BMC Pregnancy Childbirth. 2021 Feb 23;21(1):160. PubMed | Google Scholar
- Fondjo L, Boamah V, Fierti A, Gyesi D, Owiredu E. Knowledge of preeclampsia and its associated factors among pregnant women: a possible link to reduce related adverse outcomes. BMC Pregnancy Childbirth. 2019 Dec 2;19(1):456. PubMed | Google Scholar
- Lori JR, Dahlem CH, Ackah JV, Adanu RM. Examining antenatal health literacy in Ghana. J Nurs Scholarsh. 2014 Nov;46(6):432-40. PubMed | Google Scholar
- Vasquez L, PulidoAcuna C, Montanez GC, Alexandre R. Hazard deaths and sequels: perception on severe pre-eclampsia by those who lived it. Enfermeria Global. 2014;34:493-503. Google Scholar
- Vata PK, Chauhan NM, Nallathambi A, Hussein F. Assessment of prevalence of preeclampsia from Dilla region of Ethiopia. BMC Res Notes. 2015;8:816. PubMed | Google Scholar
- Khowaja AR, Qureshi RN, Sheikh S, Zaidi S, Salam R, Sawchuck D et al. Community´s perceptions of preeclampsia and eclampsia in Sindh Pakistan: a qualitative study. Reproductive Health. 2016;13((Suppl 1)):36. PubMed | Google Scholar
- Khowaja AR, Qureshi RN, Sheikh S, Zaidi S, Salam R, Sawchuck D et al. Community's perceptions of pre-eclampsia and eclampsia in Sindh Pakistan: A qualitative study. Reprod Health. 2016 Jun 8;13 Suppl 1(Suppl 1):36. PubMed | Google Scholar
- Khowaja AR, Qureshi RN, Sheikh S, Zaidi S, Salam R, Sawchuck D et al. Knowledge of hypertensive disorders of pregnancy among pregnant women attending antenatal clinic at a tertiary hospital in Ghana. SAGE Open Med. 2022 Mar 21:10:20503121221088432. PubMed | Google Scholar
- Mannava P, Durrant K, Fisher J, Chersich M, Luchters S. Attitudes and behaviors of maternal health care providers in interactions with clients: a systematic review. Global Health. 2015 Aug 15:11:36. PubMed | Google Scholar
- Areru HA, Dangisso MH, Lindtjørn B. Births and deaths in Sidama in southern Ethiopia: findings from the 2018 Dale-Wonsho Health and Demographic Surveillance System (HDSS), Global Health Action. 2020;13:1. PubMed | Google Scholar
- Lawan UM, Takai IU, Ishaq H. Perceptions about Eclampsia, Birth Preparedness, and Complications Readiness among Antenatal Clients Attending a Specialist Hospital in Kano, Nigeria. J Trop Med. 2015;2015:431368. PubMed | Google Scholar
- Yeates K, Chard S, Eberle A, Lucchese A, Chelva M, Kaushal S et al. 'They say she is bewitched': A qualitative study of community and health provider perspectives regarding pre-eclampsia and eclampsia in rural Tanzania. African Journal of Reproductive Health. 2021 Jun 1;25:92-104. Google Scholar
- Akeju DO, Vidler M, Oladapo OT, Sawchuck D, Qureshi R, von Dadelszen P et al. Community perceptions of preeclampsia and eclampsia in Ogun State, Nigeria: a qualitative study. Reproductive Health. 2016;13((Suppl 1)):57. PubMed | Google Scholar
- Tarekegn SM, Lieberman LS, Giedraitis V. Determinants of maternal health service utilization in Ethiopia: analysis of the 2011 Ethiopian Demographic and Health Survey. BMC Pregnancy and Childbirth. 2014;14(161). PubMed | Google Scholar
- Sumankuuro J, Crockett J, Wang S. Factors influencing knowledge and practice of birth preparedness and complication readiness in sub-saharan Africa: a narrative review of cross-sectional studies. International Journal of Community Medicine and Public Health. 2016 Dec;3(12):3297-307. Google Scholar
- Lefèvre GN, Berkane SU, Etienne J. Preeclampsia and oxygen free radicals. Ann Biol Clin (Paris). 1997 Sep-Oct;55(5):443-50. PubMed | Google Scholar
- Mrisho M, Obrist B, Schellenberg JA, Haws RA, Mushi AK, Mshinda H et al. The use of antenatal and postnatal care: perspectives and experiences of women and health care providers in rural southern Tanzania. BMC Pregnancy Childbirth. 2009;9:10. PubMed | Google Scholar
- Nabulo H, Ruzaaza G, Mugabi F, Bajunirwe F. Perceptions on preeclampsia and eclampsia among senior, older women, in rural Southwestern Uganda. Journal of Global Health Reports. 2021;5:e2021009. PubMed | Google Scholar
- Gebremariam LW, Aoyama A, Kahsay AB, Hirakawa Y, Chiang C, Yatsuya H et al. Perception and practice of ´healthy´ diet in relation to noncommunicable diseases among the urban and rural people in northern Ethiopia: a community-based qualitative study. Nagoya J Med Sci. 2018;80(451-464). PubMed | Google Scholar
- Ejike DE, Ambrose B, Moses DA, Karimah MR, Iliya E, Sheu OS et al. Determination, knowledge and prevalence of pregnancy-induced hypertension/eclampsia among women of childbearing age at Same District Hospital in Tanzania. International Journal of Medicine Medical Sciences. 2018;10(2):19-26. Google Scholar
- Mathole T, Lindmark G, Majoko F, Ahlberg BM. A qualitative study of women's perspectives of antenatal care in a rural area of Zimbabwe. Midwifery. 2004;20(2):122-32. PubMed | Google Scholar
- Zewdneh Shewamene, Tinashe Dune, Caroline A. Smith. The use of traditional medicine in maternity care among African women in Africa and the diaspora: a systematic review. BMC Complementary and Alternative Medicine. 2017;17(382). PubMed | Google Scholar
- Hasan IJ, Nisar N. Womens´ perceptions regarding obstetric complications and care in a poor fishing community in Karachi. J Pak Med Assoc. 2002 Apr;52(4):148-52. PubMed | Google Scholar
- Kyung-Sook Bang, Sun-Mi Chae, Insook Lee, Juyoun Yu, Jandi Kim. Effects of a Community Outreach Program for Maternal Health and Family Planning in Tigray, Ethiopia. Asian Nurs Res (Korean Soc Nurs Sci). 2018 Sep;12(3):223-230. PubMed | Google Scholar
Search

This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures
Article metrics
Recently from the PAMJ-CM






